This post rings in another new video to add to the series on the All Things Neonatal YouTube channel. I hope that you have gotten something out of the ones posted so far and that this adds something further to your approach to neonatal care.
The Golden Hour Revisited
In the last post to the video selections entitled A Golden Opportunity For Your NICU Team! the main thrust of the video was on the use of the Golden Hour approach to starting a baby on CPAP. Having a standardized checklist based approach to providing care to high risk newborns improves team functioning for sure. What do you do though when you need to hand off a patient to another team? Depending on where you work this may not be an issue if the team performing the resuscitation is the team providing the care for the patient in the NICU. Perhaps you work in a centre similar to our own where the team performing resuscitation is not the same as the one who will ultimately admit the patient. You may also be in a location where there are no babies born on site but rather all patients are transferred in so in each case the patient is new to everyone on the receiving team. How do you ensure that a complete hand over is done.
Out with the old and in with the new!
By no means do I want to imply that it is not possible to transfer information outside of the way that we demonstrate in this video. What I do believe though is that with telehealth being available in more and more settings or without a formal support for the same, the use of smartphones make video conferencing a reality for almost everyone. In most centres handovers have followed the practice of like communicating with like. Nurses give report to nurses, respiratory therapists to each other and MDs to MDs. What if there was another way though? In the video below we demonstrate another approach. Would it work for your team?
As you can tell I am a big fan of simulation in helping to create high functioning teams! More of these videos can be accessed on my Youtube channel at
The importance of collaborating in a respectful manner cannot be overemphasized, as a calm and well prepared team can handle just about anything thrown their way. This past week I finally had the opportunity to take the 7th ed NRP instructor course. What struck me most about the new version of the course was not the approach to the actual resuscitation but the preparation that was emphasized before you even start! It only takes 30 seconds to establish who is doing what in a resuscitation and while it would seem logical to divide up the roles each will take on it is something that has not been consistently done (at least in our institution). When a baby is born and responds to PPV quickly, this may not seem that important but in a situation where a team is performing chest compressions, placing an emergency UVC and moving on to epinephrine administration it certainly is nice to know in advance who is doing what.
The Golden Hour
We and many other centres have adopted this approach to resuscitation and at least here developed a checklist to ensure that everyone is prepared for a high risk delivery. While teams may think they have all the bases covered, when heart rates are racing it may surprise you to see how many times crucial bits of information or planning is missed. As I told you in another post I will be releasing a series of videos that I hope others will find useful. The video in this case is of a team readying itself for the delivery of a preterm infant that they anticipate will have respiratory distress. Ask yourself as you watch the film whether your team is preparing to this degree or not. Preparing in such a fashion certainly reduces the risk of errors caused by assumptions about who is doing what or what risk factors are present.
As you can tell I am a big fan of simulation in helping to create high functioning teams! More of these videos can be accessed on my Youtube channel at
The other day I met with some colleagues from Obstetrics and other members from Neonatology to look at a new way of configuring our delivery suites. The question on the table was which deliveries which were always the domain of the high risk labour floor could be safely done in a lower acuity area. From a delivery standpoint they would have all the tools they need but issues might arise from a resuscitation point of view if more advanced resuscitation was needed. Would you have enough space for a full team, would all the equipment you need be available and overall what is in the best interests of the baby and family?
We looked at a longstanding list of conditions both antenatal and intrapartum and one by one tried to decide whether all of these were high risk or if some were more moderate. Could one predict based on a condition how much resuscitation they might need? As we worked our way through the list there was much discussion but in the end we were left with expert opinion as there was really no data to go by. For example, when the topic of IUGR infants came up we pooled our collective experience and all agreed that most of the time these babies seem to go quite well. After a few shoulder shrugs we were left feeling good about our decision to allow them to deliver in the new area. Now several days later I have some concern that our thinking was a little too simple. You see, conditions such as IUGR may present as the only risk factor for an adverse outcome but what if they also present with meconium or the need for a instrument assisted delivery. We would presume the risk for advanced resuscitation (meaning intubation or chest compressions and/or medication need) would be increased but is there a better way of predicting the extent of this risk?
Indeed there might just be
An interesting approach to answer this question has been taken by an Argentinian group in their paper Risk factors for advanced resuscitation in term and near-term infants: a case–control study. They chose to use a prospective case control study matching one case to 4 control infants who did not require resuscitation. The inclusion criteria were fairly straightforward. All babies had to be 34 weeks gestational age or greater and free of congenital malformations. By performing the study in 16 centres they were able to amass 61953 deliveries and for each case they found (N=196) they found 784 deliveries that were matched by day of birth. The idea here was that by matching consecutive patients who did not require resuscitation you were standardizing the teams that were present at delivery.
The antepartum and intrapartum risk factors that were then examined to determine strengths of association with need for resuscitation were obtained from the list of risks as per the NRP recommendations.
A Tool For All of Us?
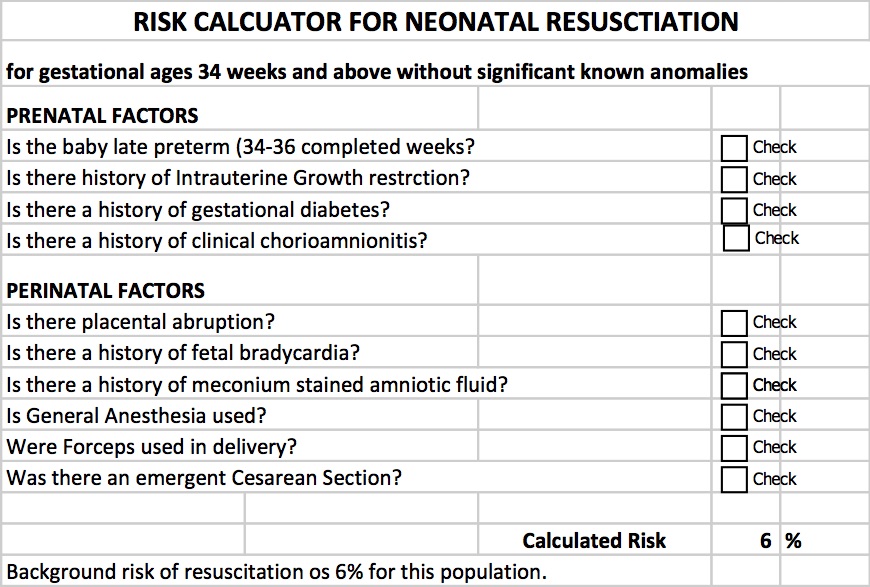
What came out of their study was a simple yet effective tool that can help to predict the likelihood of a baby needing resuscitation when all factors are taken into account. By resuscitation the authors defined this as intubation, chest compressions or medications. This is pretty advanced resuscitation! In essence this is a tool that could help us answer the questions above with far better estimation than a shoulder shrug and an “I think so” response. The table can be found by clicking on this link to download but the table looks like this.
By inserting checks into the applicable boxes you get a calculated expected need for resuscitation. Let’s look at the example that I outlined at the start of the discussion which was an IUGR infant. It turns out that IUGR itself increases the background risk for infants 34 weeks and above from 6% to 55% with that one factor alone. Add in the presence of fetal bradycardia that is so often seen with each contraction in these babies and the risk increases to 97%! Based on these numbers I would be hesitant to say that most of these kids should do well. The majority in fact would seem to need some help to transition into this world.
Some words of caution
The definition here of resuscitation was intubation, chest compressions or medications. I would like to presume that the practioners in these centres were using NRP so with respect to chest compressions and medication use I would think this should be comparable to a centre such as ours. What I don’t know for sure is how quickly these centres move to intubate. NRP has always been fairly clear that infants may be intubated at several time points during a resuscitation although recent changes to NRP have put more emphasis on the use of CPAP to establish FRC and avoid intubation. Having said that this study took place from 2011 – 2013 so earlier than the push for CPAP began. I have to wonder what the effect of having an earlier approach to intubating might have had on these results. I can only speculate but perhaps it is irrelevant to some degree as even if in many cases these babies did not need intubation now they still would have likely needed CPAP. The need for any respiratory support adds a respiratory therapist into the mix which in a crowded space with the additional equipment needed makes a small room even smaller. Therefore while I may question the threshold to intubate I suspect these results are fairly applicable in at least picking out the likelihood of needing a Neonatal team in attendance.
Moreover I think we might have a quick tool on our hands for our Obstetrical colleagues to triage which deliveries they should really have us at. A tool that estimates the risk may be better than a shoulder shrug even if it overestimates when the goal is to ensure safety.
As I was preparing to settle in tonight I received a question from a reader on my Linkedin page in regards to the use of sustained inflation (SI) in our units. We don’t use it and I think the reasons behind it might be of interest to others. The concept of SI is that by providing a high opening pressure of 20 – 30 cm H2O for anywhere from 5 to 15 seconds one may be able to open the “stiff” lung of a preterm infant with RDS and establish an adequate functional residual capacity. Once the lung is open, it may be possible in theory to keep it open with ongoing peep at a more traditional level of 5 – 8 cm of H20.
The concept was tested 25 years ago by Vyas et al in their article Physiologic responses to prolonged and slow-rise inflation in the resuscitation of the asphyxiated newborn infant. In this study, 9 newborn infants were given a relatively short 5 second sustained inflation and led to earlier and larger lung volumes with good establishment of FRC. Like many trials in Neonatology though sceptics abound and here we are 25 years later still discussing the merits of this approach.
As I have a warm place in my heart for the place that started my professional career whenever I come across a paper published by former colleagues I take a closer look. Such is the case with a systematic review on sustained inflation by Schmolzer et al. The inclusion criteria were studies of infants born at <33 weeks. Their article provides a wonderful assessment of the state of the literature on the topic and I would encourage you to have a look at it if you would like a good reference to keep around on the topic. What it comes down to though is that there are really only four randomized human studies using the technique and in truth they are fairly heterogeneous in their design. They vary in the length of time an SI was performed (5 – 20 seconds), the pressures used (20 – 30 cm H2O), single or multiple SIs and lastly amount of oxygen utilized being 21 – 100%. In fact three of the four studies used either 100% or in one case 50% FiO2 when providing such treatments.
What Did They Show?
This is where things get interesting. SI works in the short term by reducing the likelihood that an infant will need mechanical ventilation at 72 hours with a number needed to treat of only 10! In medicine we normally would embrace such results but sadly the results do not translate into long term benefits as the rate of BPD, mortality and the combined outcome do not remain significant. Interestingly, the incidence of a symptomatic PDA needing treatment with either a medical or surgical approach had a number needed to harm of 11; an equally impressive number but one that gives reason for concern. As the authors speculate, the increased rate of PDA may be in fact related to the good job that the SI does in this early phase. By establishing an open lung and at an earlier time point it may well be that there is an accentuation in the relaxation of the pulmonary vasculature and this leads to a left to right shunt that by being hemodynamically significant helps to stent the ductus open at a time when it might otherwise be tending to close. This outcome in and of itself raises concern in my mind and is the first reason to give me reason to pause before adopting this practice.
Any other concerns?
Although non-significant there was a trend towards increased rates of IVH in the groups randomized to SI. There is real biologic plausibility here. During an SI the increased positive pressure in the chest could well simulate a similar effect to a pneumothorax and impede the passive drainage of blood from the head into the thorax. In particular, longer durations and/or frequent SIs could increase such risk. Given the heterogeneous nature of these studies it is difficult to know if they all had been similar in providing multiple SIs could we have seen this cross over to significant?
I believe the biggest concern in all of this though is that I would have a very hard time applying the results of these studies to our patient population. The systematic review addresses the question about whether SI is better than IPPV as a lung recruitment strategy in the preterm infant with respiratory distress. I have to say though we have moved beyond IPPV as an initial strategy in favour of placement of CPAP on the infant directly after birth. The real question in my mind is whether providing brief periods of SI followed by CPAP of +6 to +8 is better than placement on CPAP alone as a first strategy to establish good lung volumes.
If I am to be swayed by the use of SI someone needs to do this study first. The possibility of increasing the number of hemodynamically significant PDAs and potentially worsening IVH without any clear reduction in BPD is definitely placing me firmly in the camp of favouring the CPAP approach. Having said all that, the work by the Edmonton group is important and gives everyone a glimpse into what the current landscape is for research in this field and opens the door for their group or another to answer my questions and any others that may emerge as this strategy will no doubt be discussed for years to come.
Ask almost anyone who has worked in the field of Neonatology for some time and they will tell you that babies are not as sick as they once were. We can give a lot of credit to better antenatal steroid use, maternal nutrition and general management during pregnancy. Additionally, after birth we now rush to place infants on CPAP and achieve adequate expansion of the lungs which in many cases staves off intubation.
The downside to our success though is that the opportunities to provide positive pressure ventilation (PPV) and moreover intubation are becoming less and less. How then do we perform when we are asked to do such procedures on an infrequent basis? The answer as you might expect is not that well. Dr. Schmolzer et al studied the ability of people to keep a good seal and found a 29% leak on average with as high as 63% in one patient. As this was a study in which people were being observed one might think the Hawthorne Effect might artificially decrease the percentage leak compared to real world scenarios when you know you aren’t being watched.
What is the cause of the leak?
Leaks most commonly occur on either side of the nasolabial folds. Although at least in my experience we educate trainees about this issue it remains a problem. I would also speculate that at the times when we need to be at our best during an advanced resuscitation involving chest compressions we may well function at our worst. This is the effect of the adrenalin rushing through our system as our sympathetic system turns into overdrive. The question therefore is one of getting around human error in particular when we need to minimize such inefficiency the most.
The Solution?
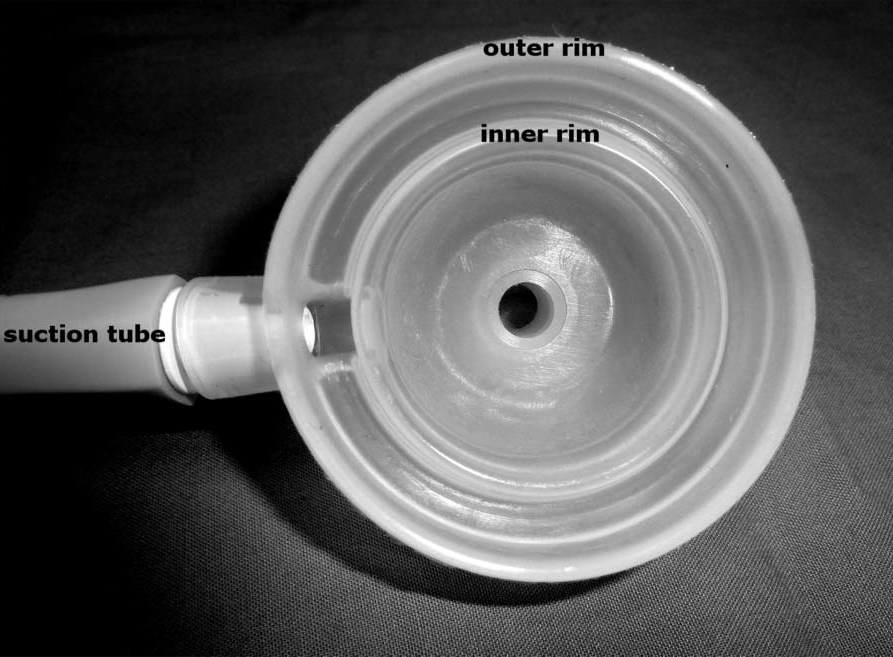
If the masks are prone to leaking and with it the ability to properly ventilate compromised, how could we minimize such human error. The answer may lie in what I consider to be an ingenious way to apply a mask. The concept and it is just that at the moment is to use suction to apply the mask to the face without risk of leak. Lorenz L et al have just published a proof of concept study utilizing a mannequin with a “seal skin” layer applied to the face to simulate human skin. The article is entitled A new suction mask to reduce leak during neonatal resuscitation: a manikin study.
In this study, the mask was applied to the face of the mannequin and 100 cm H2O pressure was applied through a side port on the mask. There is an inner and outer ring such that the internal 41 mm diameter mask is surrounded by a double wall in which the suction is applied to the space between the two walls leading to the mask seating itself firmly against the face. The authors then studied the amount of leak found when using a Neopuff set to deliver 40 – 60 breaths per minute at pressures of 25/5. For this study 60 courses were tested.
How did it do compared to PPV through a traditional mask?
As you might expect (since you can feel my excitement!) it did very well. The average leaks using a conventional approach were quite good at 12.1% but the suction mask was only 0.7% leak. Importantly the ranges were quite different. PPV through a conventional mask had a range of 0.6 – 39% leak while with the suction version it was 0.2 – 4.6%. These results were statistically different.
What does the future hold?
As mentioned this study is what one would consider a proof of concept study. We do not know how this would fare in the real world and that of course is the next step. In terms of harm, the authors did note that when applied to the forearm of an adult it caused some mild redness from the suction that vanished quickly on breaking of the seal but we do not know if there could be greater harm in a newborn in particular one who is quite small. Such testing will be needed as part of any further study.
Having said that I think this rethink of the mask for PPV could be transformative to those who perform neonatal resuscitation infrequently. If this mask is found not only to be effective in a clinical trial but safe as well I would suggest a change to this type of mask could quite literally be life saving. Placed in the hands of those who are inexperienced in keeping a seal, PPV would become much more effective and in particular for rural sites the infants being transported in much more stable than some are at present.
Keep your eyes peeled for future work using this mask. Something tells me if it proves to be efficacious outside of a seal skin covered mannequin, your toolkit for providing NRP may be in for a change.
Every now and then I come across an instance when I discover that something that I have known for some time truly is not as well appreciated as I might think.
Twice in my career I have come across the following situation which has been generalized to eliminate any specific details about a patient. In essence this is a fictional story but the conclusions are quite real.
Case of the Flat Baby
A mother arrives at the hospital with severe abdominal pain and in short order is diagnosed with a likely abruption at 26 weeks gestational age. Fetal monitors are attached and reveal a significant fetal bradycardia with a prolonged period of minutes below 100 and sometimes below 60 beats per minute. She is rushed to the OR where an emergency c-section is performed.
A live born infant is handed to the resuscitation team after cord clamping is stopped at 30 seconds due to significant cyanosis and no respirations. After placing the infant in a polyethylene wrap and performing the initial steps of ventilation there is no respiratory effort and the baby is given PPV. After no heart rate is noted chest compressions commence followed by intubation and then epinephrine when a heart rate while detected remains below 60. The team gives a bolus of saline followed by another round of epinephrine and by 10 minutes a pulse of 80 BPM is detected. While a pulse is present it remains borderline and the baby shows no sign of any respiratory efforts.
The care providers at this point have a decision to make about continuing resuscitative efforts or not. One of the team members performs a physical exam at this stage and notes that the pupils are unresponsive to light with a 3 mm pupillary diameter. The team questions whether based on this finding irreversible neurological damage has occurred.
Pupillary Reactions in Preterm Infants
It turns out that much like many organs in the body which have yet to fully mature the same applies to the eye or more specifically in this case the pupil. Robinson studied 50 preterm infants in 1990 and noted that none of the infants under 30 weeks gestational age demonstrated any reaction to light shone in the eye. After 30 weeks the infants gradually realized this function until by 35 weeks all infants had attained this pupillary reaction to light.
Isenberg in the same year when examining 30 preterm infants under 30 weeks noted that in addition to the lack of pupillary constriction to light, as the gestational age decreased the pupillary diameter enlarged. The youngest infants in this study at 26 weeks had a mean pupillary diameter of 4.7 mm while by 29 weeks this number decreased to 2.9 mm. This means that the smaller the infant the larger the pupillary size and given that these are also the highest risk infants one can see how the appearance of a “fixed and dilated pupil” could lead one down the wrong path.
Conclusion
Deciding when to stop a resuscitation is never an easy decision. Add to this as I recently wrote, even after 10 minutes of resuscitation outcomes may not be as bad as we have thought; Apgar score of 0 at 10 minutes: Why the new NRP recommendations missed the mark. What I can say and obviously was the main thrust of this piece is that at least when you are resuscitating an infant < 30 weeks gestational age, leave the eyes out of the decision. The eyes in this case “do not have it”.


 The importance of collaborating in a respectful manner cannot be overemphasized, as a calm and well prepared team can handle just about anything thrown their way. This past week I finally had the opportunity to take the 7th ed NRP instructor course. What struck me most about the new version of the course was not the approach to the actual resuscitation but the preparation that was emphasized before you even start! It only takes 30 seconds to establish who is doing what in a resuscitation and while it would seem logical to divide up the roles each will take on it is something that has not been consistently done (at least in our institution). When a baby is born and responds to PPV quickly, this may not seem that important but in a situation where a team is performing chest compressions, placing an emergency UVC and moving on to epinephrine administration it certainly is nice to know in advance who is doing what.
The importance of collaborating in a respectful manner cannot be overemphasized, as a calm and well prepared team can handle just about anything thrown their way. This past week I finally had the opportunity to take the 7th ed NRP instructor course. What struck me most about the new version of the course was not the approach to the actual resuscitation but the preparation that was emphasized before you even start! It only takes 30 seconds to establish who is doing what in a resuscitation and while it would seem logical to divide up the roles each will take on it is something that has not been consistently done (at least in our institution). When a baby is born and responds to PPV quickly, this may not seem that important but in a situation where a team is performing chest compressions, placing an emergency UVC and moving on to epinephrine administration it certainly is nice to know in advance who is doing what.

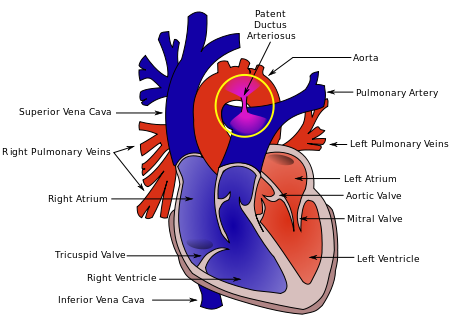 As the authors speculate, the increased rate of PDA may be in fact related to the good job that the SI does in this early phase. By establishing an open lung and at an earlier time point it may well be that there is an accentuation in the relaxation of the pulmonary vasculature and this leads to a left to right shunt that by being hemodynamically significant helps to stent the ductus open at a time when it might otherwise be tending to close. This outcome in and of itself raises concern in my mind and is the first reason to give me reason to pause before adopting this practice.
As the authors speculate, the increased rate of PDA may be in fact related to the good job that the SI does in this early phase. By establishing an open lung and at an earlier time point it may well be that there is an accentuation in the relaxation of the pulmonary vasculature and this leads to a left to right shunt that by being hemodynamically significant helps to stent the ductus open at a time when it might otherwise be tending to close. This outcome in and of itself raises concern in my mind and is the first reason to give me reason to pause before adopting this practice.
 Lorenz L et al have just published a proof of concept study utilizing a mannequin with a “seal skin” layer applied to the face to simulate human skin. The article is entitled
Lorenz L et al have just published a proof of concept study utilizing a mannequin with a “seal skin” layer applied to the face to simulate human skin. The article is entitled 
