I couldn’t think of a better topic for World Prematurity Day 2021 than what constitutes the edge of viability. Thinking back over my career, when I was a resident and fellow infants born at 25 and 26 weeks were deemed about as low as “we should” go but we certainly resuscitated infants at 24 weeks but this was considered heroic. Jump ahead to the last decade and we began caring for infants at birth at 23 weeks so commonly that the thought of offering comfort care only to infants at 24 weeks became almost unthinkable for many health care providers. Before I get jumped on, let me say that I am not saying I agree or disagree with that sentiment but it is something that is felt by many.
The Shared Decision Model
In the last few years a rethink again has occurred whereby the concept of the treating team knowing best has been replaced by the “shared decision model”. In this line of thinking, it is not up to us as health care providers to “tell the parents” what to do but rather come to a shared decision based on an assessment of the wishes and values of the parents in conjunction with hearing about both short and long term problems their infants may face if resuscitated. This concept was central to the statement by the Canadian Pediatric Society that I am proud to have been part of with respect to its development. The statement for those that are interested is Counselling and management for anticipated extremely preterm birth
What’s next? Going below 22 weeks?
The challenge of the shared decision model is that there comes a point where the answer is simply “no”. If for example a family at 19 weeks gestation demanded an attempt at resuscitation I would have to inform them that survival is not possible (assuming ultrasound confirmed anthropometric measurements consistent with that age). The question though becomes a little more difficult to answer at 21 weeks and was the subject of a recent article in the New York Times about a survivor at 21 weeks gestation.
Even with the best gestational age dating the estimate can be off by up to 5 days so it’s possible that the infant in this story was closer to 22 weeks or even midpoint between 22 and 23 weeks in reality. Regardless it does raise the question about what to do at 21 weeks and I suspect we will begin to see more stories about this now that the glass ceiling of 22 weeks has been breached. What about below 21 weeks? Sounds impossible I know but with research that remains at the stage of animal studies this may become possible. Maybe not in the next 5-10 years but it could happen in my lifetime in this chosen field.
The Artificial Placenta
This made headlines a few years ago with the news that the Children’s Hospital of Philadelphia had successfully kept a lamb alive for a period of 4 weeks using an artificial placenta and amniotic fluid.
You might think that this was a one-off experiment that will never see the light of day but similar work is being done in Toronto, Canada where they have been able to do similar work with preterm piglets in their paper Achieving sustained extrauterine life: Challenges of an artificial placenta in fetal pigs as a model of the preterm human fetus. Incidentally as my colleague Dr. Ayman Sheta worked on this project while in Toronto I am particularly pleased to share this research. Similar to the experience in CHOP the team in Toronto has been able to keep piglets alive for progressively longer durations. My understanding is that despite the best efforts infectious complications over arise limiting how long one can sustain such animals.
This leads me to my final thoughts on where we might be able to go. I see a future where we apply such technology to humans but not in the way that people might have thought. Keeping a fetus after delivery at 21 or 20 weeks on an artificial placenta for many weeks is not likely a realistic goal. What if we could get 1 or 2 weeks though and allow the fetus to be oxygenated without using positive pressure on their developing lungs and transition them at 23 or 24 weeks gestation? We may in this way be able to allow for postnatal maturation in a artificial uterine environment and give babies a chance who would otherwise never had the opportunity for a shared decision with medical staff.
Sound like science fiction? Well the beauty of the internet as my friend told me today is that once it’s out there it out there for good. Let’s see how this post stands the test of time and to all the babies out there in NICUs and to their families I wish you all a good and uneventful World Prematurity Day wherever you may be!
Inhaled nitric oxide has been around for some time now. I recall it being called at one point in medical school “endothelial relaxation factor” and then later on identified as nitric oxide. Many years later it finds itself in common usage in NICUs all over the world. Our experience though has been for treatment of pulmonary hypertension and for that it is pretty clear that for those afflicted by that condition it can be lifesaving. Over the years other uses have been looked at including prevention of BPD (turned out not to be the case). Rescue approaches therefore have found to be useful but on the prophylactic side of things not so much.
Maybe starting earlier is the key?
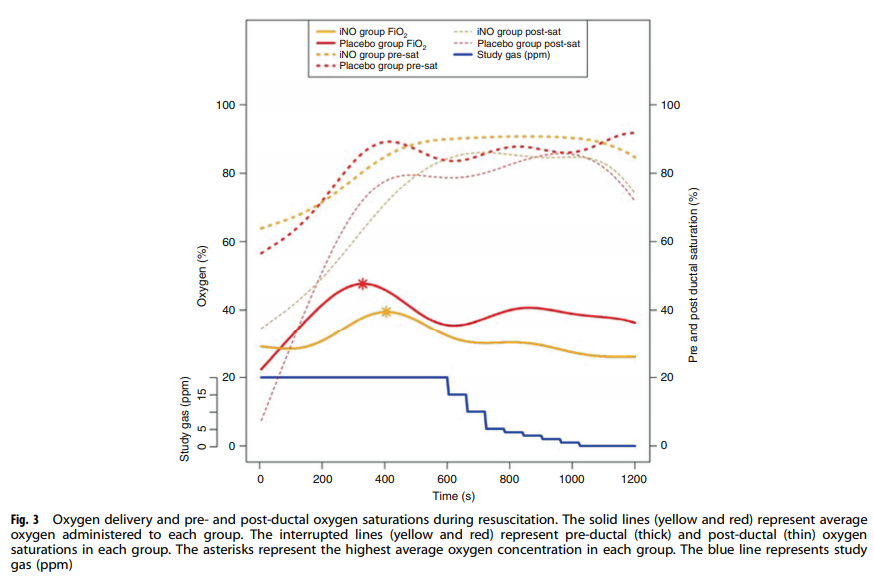
A group based out of Oklahoma has published a pilot study that raised an eyebrow for me at least. Krishnamurthy et al released Inhaled Nitric Oxide as an Adjunct to Neonatal Resuscitation in Premature Infants: A pilot, double blind, randomized controlled trial . The study set out to recruit 40 infants who between 30-90 seconds of life if requiring PPV would either get iNO 20 ppm with 30% oxygen or 30% oxygen and placebo for ten minutes. At ten minutes weaning of iNO by 1 ppm per minute for a total of 17 minutes was done. The primary outcome of interest was FiO2 required to achieve target oxygen saturations. As with many studies that seek enrollment prior to delivery this study was a challenge as well with early termination of the study after 28 babies (14 in each group) were recruited.
Did they find anything interesting?
In spite of the low numbers in the study, the authors did find a divergence in the FiO2 needed to achieve the target oxygen saturations.
The authors conclusions were that the cumulative exposure to FiO2 was lower in the iNO group as well as the maximum exposed FiO2 of 39% vs 48% (although this almost but not quite met statistical significance. Even then this is a pilot study so inferring too much could be a dangerous thing.
The study though does get one thinking but we need to be wary of letting our brains do some mental trickery. Lower FiO2 seems like a good thing given what we know about oxygen free radicals. What about rapid lowering of pulmonary vascular resistance with exogenous iNO? Is this a good thing or could other things be lurking around the corner? Could a larger study for example find a higher rate of pulmonary hemorrhage with rapid reductions in PVR? The authors did not find harm in the study but again with small numbers it is hard to conclude too much.
What this small study does though is raise many questions that I think could be interesting to answer. If a patient needs less FiO2 at 17 minutes after study entry might there be less perceived need for higher PEEP if ventilated or CPAP levels if on non-invasive support? Less pressure could lead to less risk of pneumothorax (or more perhaps if under treated but with respiratory distress. Less pressure might also influence longer term risks of BPD from barotrauma or volutrauma for that matter.
Regardless this is only the beginning. I have no doubt there will be further trials on the way. The trick will be as in this study to obtain consent unless a deferred consent could be obtained but I have my doubts about getting that. Nonetheless, wait for more to come!
Recent statements by the American Academy of Pediatric’s, NICHD, the American College of Obstetricians and Gynecologists (ACOG), the Society for Maternal-Fetal Medicine (SMFM), and recommend selective approaches to mothers presenting between 22 0/7 to 22 6/7 weeks. The decision to provide antenatal steroids is only recommended if delivery is expected after 23 weeks. Furthermore the decision to resuscitate is based on an examination of a number of factors including a shared decision with the family. In practice this leads to those centres believing this is mostly futile generally not resuscitating or offering steroids while other more optimistic hospitals having higher rates of proactive (steroids and resuscitation) rates. Then there are other centres where the standard approach is proactive such as one in Uppsala, Sweden where this approach is used almost exclusively.
What would happen then if one compared the outcome for infants born at 22 weeks between this hospital and another where a selective approach is generally offered. In this case you would have a lot of experience with resuscitating infants at 22 weeks and the other a fraction of all presenting as a few to many would receive compassionate care. This is exactly what has now happened.
A Tale of Two Cities
The University Children’s Hospital, Uppsala, Sweden has been compared retrospectively to Nationwide Children’s Hospital, Columbus, Ohio, USA (NCH) with respect to survival and outcomes for their infants born at 22 weeks. The paper by Backes CH et al entitled Outcomes following a comprehensive versus a selective approach for infants born at 22 weeks of gestation tells a very interesting story about the power of belief or faith that one can accomplish something if they set their mind to it.
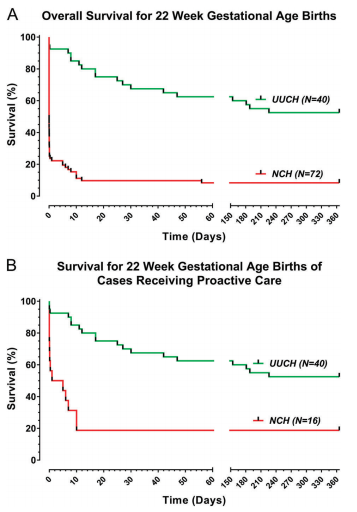
The authors examined a period from 2006-2015, dividing this time into two epochs with the first being 2006-2010 to account for differing practices and resources over time. Given that Uppsala took a proactive approach to all of their 40 live born infants during this time, it provided an opportunity to look at the 72 infants who were live born in the Ohio and examine their differences. In Ohio the approach was as follows; 16 (22%) received proactive care, 18 (25%) received inconsistent care (steroids but no resuscitation), and 38 (53%) received comfort care. In other words, although the total number of infants live born in Ohio was almost double that of Uppsala, only 16 were proactively treated in Ohio compared to all 40 in Uppsala.
The differences in outcome are striking
Survival in delivery room: (38/40, 95% vs 12/16, 75%; P = 0.049)
Provision of delivery room surfactant: (40/40, 100% vs 9/16, 56%; P<0.01)
Survival at 24 h (37/40, 93% vs. 9/16, 56%; P < 0.01).
Survival to 1 year (21/40, 53% vs. 3/16, 19%; P < 0.05).
Among the infants treated proactively, median age of death (17 postnatal days at range 0 h–226 days vs. 3 postnatal hours at NCH, range 0 h–10 days; P < 0.01).
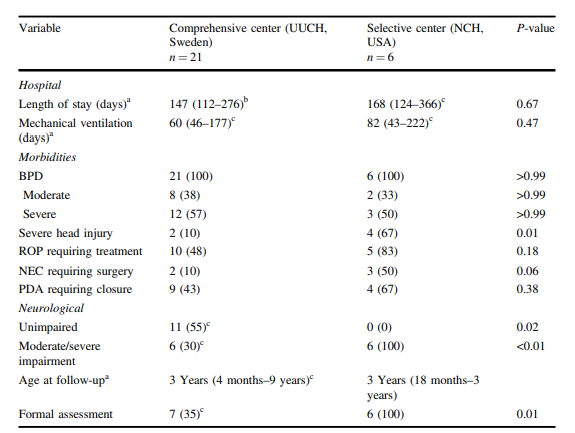
All surviving infants had BPD All infants surviving to initial hospital discharge were alive at 18 months’ postnatal age.
With respect to long term outcome the authors note:
“Outpatient follow-up (qualitative or non-qualitative neurodevelopmental testing) was available in 26 out of 27 infants (96%) Eleven of the 26 (42%) were unimpaired, and all unimpaired infants were in the UUCH cohort. Among the 15 infants with impairment at UUCH, 3 had mild impairment and 12 had moderate or severe impairment. All surviving infants at NCH had moderate or severe impairment.”
A word about antenatal steroids as well. In Uppsala 85% of mothers received 2 doses of antenatal steroids vs 25% in Ohio. People sometimes question whether ANS at this age are effective. It is interesting to note that 44% of babies in the Ohio group vs 3% p<0.01 received chest compressions +/- epinephrine in the delivery room. Might this explain the better state of some of these infants at birth?
The Power of Belief
When I do rounds I often remark that try as we might we can’t will babies to do better. I also commonly say however that we need to be optimistic and although I am accused of seeing the world through rose coloured glasses I think there is an important lesson to be learned from this study. This comparison is really a contrast between a system that believes they can do a good thing for these families by actively promoting a proactive approach vs a system in which I imagine a reluctant approach exists even for those infants where a proactive plan is enacted. One sign of this might be that in Sweden 100% of these deliveries had a Neonatologist present vs 75% in the US. It could be due to other factors such as ability of the Neo to get in within time of the delivery however rather than a sign they didn’t feel they were needed due to futility.
There is evidence as well that the aggressiveness of the proactive approach also differs between the two sites based on a couple observations. The first is the rate of surfactant provision in the delivery room which was 100% in Sweden but only 56% in the US. The other thing of note is the time of death for those who did not survive. The median time of death in the US was 3 hours vs 17 days in Uppsala. What does this tell us about the approaches? I would imagine (although the numbers are small) that the teams in the US were much more likely to lose hope (or faith) and withdraw early while the other centre possibility motivated by their past successes pushed forward.
Remarkably, although one might think that the teams in Uppsala were simply creating significantly impaired survivors, 42% of the survivors were unimpaired from a developmental standpoint in follow-up. All surviving infants though from Ohio had moderate to severe impairment.
What this story may also really be about is practice. The reality is that the team in Sweden had over twice the exposure to such infants over time. Although the number presenting at this GA was higher, the ones that actually were resuscitated and given steroids was less than half. One cannot take away though that Uppsala in the end demonstrated that a proactive approach is definitely not futile. Not only can these children survive but almost half will be developmentally intact.
We must acknowledge as well though that since this is a retrospective study there may be factors that may have affected the results. As the saying goes “Individual results may vary”. Are the teams the same in both centres in terms of number of Neonatologists? Are there more residents caring for these infants vs fellows? Are the resources the same? What about proximity of the Neonatologist to the hospital? There are other factors such as cohesiveness of the team and communication between team members that may be influencing the results.
In the end though, this is a story of a team that believed it could and did. Perhaps seeing the world through rose coloured glasses is not such a bad thing in the end.
A few weeks back I wrote about the topic of intubations and whether premedication is really needed (Still performing awake intubations in newborns? Maybe this will change your mind.) I was clear in my belief that it is and offered reasons why. There is another group of practitioners though that generally agree that premedication is beneficial but have a different question. Many believe that analgesia or sedation is needed but question the need for paralysis. The usual argument is that if the intubation doesn’t go well and the patient can’t spontaneously ventilate could we be worse off if the patient loses their muscle tone.
Neonatal Intubation Registry
At the CPS meeting last month in Quebec City. I had the pleasure of listening to a talk by Dr. Elizabeth Foglia on the findings from a Neonatal intubation registry that many centres have been contributing to. The National Emergency Airway Registry for Neonates (NEAR4NEOs), records all intubations from a number of centres using an online database and allows for analysis of many different aspects of intubations in neonates.
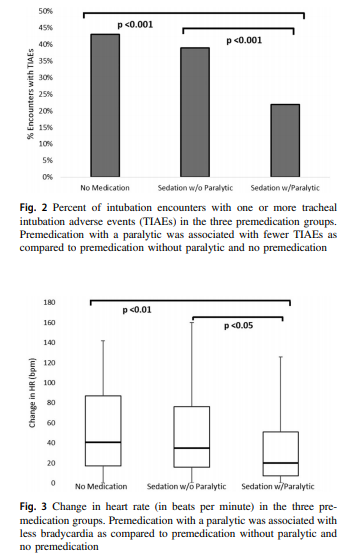
This year, J. Krick et al published Premedication with paralysis improves intubation success and decreases adverse events in very low birth weight infants: a prospective cohort study. This study compared results from the registry of two centres, the University of Washington Medical Center (UWMC) and Seattle Children’s Hospital where the former rarely uses paralysis and the latter in almost all instances of non-emergent intubation. In all, 237 encounters were analyzed in the NICU for babies < 1500g with the majority of encounters (181) being from UWMC. The median PMA at intubation was 28 completed weeks (IQR: 27, 30), chronological age was 9 days (IQR: 2, 26) and weight was 953 g (IQR: 742,1200). The babies were compared based on the following groups. Premedication with a paralytic 21%, without a paralytic 46% and no premedication 31%.
This was an observational study that examined the rates of adverse events and subdivided into severe (cardiac arrest, esophageal intubation with delayed recognition, emesis with witnessed aspiration, hypotension requiring intervention (fluid and/or vasopressors), laryngospasm, malignant hyperthermia, pneumothorax/pneumomediastinum, or direct airway injury) vs non-severe (mainstem bronchial intuba- tion, esophageal intubation with immediate recognition, emesis without aspiration, hypertension requiring therapy, epistaxis, lip trauma, gum or oral trauma, dysrhythmia, and pain and/or agitation requiring additional medication and causing a delay in intubation.).
How did the groups compare?
It turns out paralysis seems to be a big deal (at least in this group of infants). Use of paralysis resulted in less attempts to intubate (median 1 attempt; IQR: 1, 2.25 vs. 2; IQR: 1, 3, p < 0.05)). In fact success was no different between the groups with no paralysis or no premedication at all! When it comes to tracheal intubation adverse events the impact of using paralysis becomes more evident. Paralysis does make a difference in reducing the incidence of such events and moreover when only looking at the rate of severe adverse events as defined above the finding was that none occurred when paralysis was used vs 9 when no paralysis was employed and 5 when no premedication was used at all. The rate of bradycardic events was less in the paralytic group but rates of oxygen desaturation between the three arms were no different.
How do we interpret the results?
Based on the results from the registry it looks like paralysis is a good thing here when electively intubating infants. If we try to determine the reason for it I suspect it may have much to do with the higher likelihood of success on the first attempt at placing an ETT. The longer it takes to place the ETT or the more number of attempts requiring intermittent PPV in a patient who truly needs a tube the greater the likelihood that you will see adverse events including bradycardia. It may simply be that a calm and still patient is an easier intubation and getting the tube in faster yields a more stable patient.
I am biased though and I think it is worth pointing out another possible reason for the differing results. One hospital in this study routinely used premedication and the other did not. Almost 3/4 of the patients came from one hospital which raises the possibility that skill set could be playing a role. If the skill of providers at the two hospitals differed, the results could reflect the variable skill in the practitioners versus the difference in the medications used themselves. What I don’t know though is whether the two share the same training program or not. Are the trainees the same at both sites (google maps says the two sites are 11 minutes away by car)? The difference still might be in local respiratory therapists or Neonatologists intubating as well. Regardless, the study provides evidence that paralysis makes a difference. To convince those out there though who remain skeptical I think we are going to need the registry to take part in a prospective trial using many centres. A format in which several centres that don’t use paralysis are compared to several who do routinely would help to sort out the concern in skill when looking only at two centres. This wouldn’t be randomized of course but I think it would be very difficult at this point to get a centre that strongly believes in using paralysis to randomize so a prospective study using groups chosen by the individual centre might be the next best thing. If anyone using the registry is reading this let me know what you think?
If I look back on my career there have been many things I have been passionate about but the one that sticks out as the most longstanding is premedicating newborns prior to non-emergent intubation. The bolded words in the last sentence are meant to reinforce that in the setting of a newborn who is deteriorating rapidly it would be inappropriate to wait for medications to be drawn up if the infant is already experiencing severe oxygen desaturation and/or bradycardia. The CPS Fetus and Newborn committee of which I am a member has a statement on the use of premedication which seems as relevant today as when it was first developed. In this statement the suggested cocktail of atropine, fentanyl and succinylcholine is recommended and having used it in our centre I can confirm that it is effective. In spite of this recommendation by our national organization there remain those who are skeptical of the need for this altogether and then there are others who continue to search for a better cocktail. Since I am at the annual conference for the CPS in Quebec city I thought it would be appropriate to provide a few comments on this topic.
Three concerns with rapid sequence induction (RSI) for premedication before intubation
1. “I don’t need it. I don’t have any trouble intubating a newborn” – This is perhaps the most common reason I hear naysayers raise. There is no question that an 60-90 kg practitioner can overpower a < 5kg infant and in particular an ELBW infant weighing < 1 kg. This misses the point though. Premedicating has been shown to increase success on the first attempt and shorten times to intubation. Dempsey 2006, Roberts 2006, Carbajal 2007, Lemyre 2009
2. “I usually get in on the first attempt and am very slick so risk of injury is less.” Not really true overall. No doubt there are those individuals who are highly successful but overall the risk of adverse events is reduced with premedication. (Marshall 1984, Lemyre 2009). I would also proudly add another Canadian study from Edmonton by Dr. Byrne and Dr. Barrington who performed 249 consecutive intubations with predication and noted minimal side effects but high success rates at first pass.
3. “Intubation is not a painful procedure”. This one is somewhat tough to obtain a true answer for as the neonate of course cannot speak to this. There is evidence available again from Canadian colleagues in 1984 and 1989 that would suggest that infants at the very least experience discomfort or show physiologic signs of stress when intubated using an “awake” approach. In 1984 Kelly and Finer in Edmonton published Nasotracheal intubation in the neonate: physiologic responses and effects of atropine and pancuronium. This randomized study of atropine with or without pancuronium vs control demonstrated intracranial hypertension only in those infants in the control arm with premedication ameliorating this finding. Similarly, in 1989 Barrington, Finer and the late Phil Etches also in Edmonton published Succinylcholine and atropine for premedication of the newborn infant before nasotracheal intubation: a randomized, controlled trial. This small study of 20 infants demonstrated the same finding of elimination of intracranial hypertension with premedication. At the very least I would suggest that having a laryngoscope blade put in your oral cavity while awake must be uncomfortable. If you still doubt that statement ask yourself whether you would want sedation if you needed to be intubated? Still feel the same way about babies not needing any?
4. What if I sedate and paralyze and there is a critical airway? Well this one may be something to consider. If one knows there is a large mass such as a cystic hygroma it may be best to leave the sedation or at least the paralysis out. The concern though that there might be an internal mass or obstruction that we just don’t know about seems a little unfounded as a justification for avoiding medications though.
Do we have the right cocktail?
The short answer is “I don’t know”. What I do know is that the use of atropine, an opioid and a muscle relaxant seems to provide good conditions for intubating newborns. We are in the era of refinement though and as a recent paper suggests, there could be alternatives to consider;Effect of Atropine With Propofol vs Atropine With Atracurium and Sufentanil on Oxygen Desaturation in Neonates Requiring Nonemergency IntubationA Randomized Clinical Trial. I personally like the idea of a two drug combination for intubating vs.. three as it leaves one less drug to worry about a medication error with. There are many papers out there looking at different drug combinations. This one though didn’t find a difference between the two combinations in terms of prolonged desaturations between the two groups which was the primary outcome. Interestingly though the process of intubating was longer with atropine and propofol. Given some peoples reluctance to use RSI at all, any drug combination which adds time to the the procedure is unlikely to go over well. Stay tuned though as I am sure there will be many other combinations over the next few years to try out!
One of the benefits of operating this site is that I often learn from the people reading these posts as they share their perspectives. On a recent trip I was reunited with Boubou Halberg a Neonatologist from Sweden whom I hadn’t seen in many years. I missed him on my last trip to Stockholm as I couldn’t make it to Karolinska University but we managed to meet each other in the end. As we caught up and he learned that I operated this site he passed along a paper of his that left an impact on me and I thought I would share with you.
When we think about treating an infant with a medicinal product, we often think about getting the right drug, right dose and right administration (IV, IM or oral) for maximum benefit to the patient. When it comes to nutrition we have certainly come a long way and have come to rely on registered dietitians where I work to handle a lot of the planning when it comes to getting the right prescription for our patients. We seem comfortable though making some assumptions when it comes to nutrition that we would never make with respect to their drug counterparts. More on that later…
A Swedish Journey to Ponder
Westin R and colleagues (one of whom is my above acquaintance) published a seven year retrospective nutritional journey in 2017 from Stockholm entitled Improved nutrition for extremely preterm infants: A population based observational study. After recognizing that over this seven year period they had made some significant changes to the way they approached nutrition, they chose to see what effect this had on growth of their infants from 22 0/7 to 26 6/7 weeks over this time by examining four epochs (2004-5, 2006-7, 2008-9 and 2010-11. What were these changes? They are summarized beautifully in the following figure.
Not included in the figure was a progressive change as well to a more aggressive position of early nutrition in the first few days of life using higher protein, fat and calories as well as changes to the type of lipid provided being initially soy based and then changing to one primarily derived from olive oil. Protein targets in the first days to weeks climbed from the low 2s to the mid 3s in gram/kg/d while provision of lipid as an example doubled from the first epoch to the last ending with a median lipid provision in the first three days of just over 2 g/kg/d.
While figure 3 from the paper demonstrates that regardless of time period there were declines in growth across all three measurements compared to expected growth patterns, when one compares the first epoch in 2004-2005 with the last 2010-11 there were significant protective effects of the nutritional strategy in place. The anticipated growth used as a standard was based on the Fenton growth curves.
What this tells us of course is that we have improved but still have work to do. Some of the nutritional sources as well were donor breast milk and based on comments coming back from this years Pediatric Academic Society meeting we may need to improve how that is prepared as growth failure is being noted in babies who are receiving donated rather than fresh mother’s own milk. I suspect there will be more on that as time goes by.
Knowing where you started is likely critical!
One advantage they have in Sweden is that they know what is actually in the breast milk they provide. Since 1998 the babies represented in this paper have had their nutritional support directed by analyzing what is in the milk provided by an analyzer. Knowing the caloric density and content of protein, carbohydrates and fats goes a long way to providing a nutritional prescription for individual infants. This is very much personalized medicine and it would appear the Swedes are ahead of the curve when it comes to this. in our units we have long assumed a caloric density of about 68 cal/100mL. What if a mother is producing milk akin to “skim milk” while another is producing a “milkshake”. This likely explains why some babies despite us being told they should be getting enough calories just seem to fail to thrive. I can only speculate what the growth curves shown above would look like if we did the same study in units that actually take a best guess as to the nutritional content of the milk they provide.
This paper gives me hope that when it comes to nutrition we are indeed moving in the right direction as most units become more aggressive with time. What we need to do though is think about nutrition no different than writing prescriptions for the drugs we use and use as much information as we can to get the dosing right for the individual patient!







 Paralysis does make a difference in reducing the incidence of such events and moreover when only looking at the rate of severe adverse events as defined above the finding was that none occurred when paralysis was used vs 9 when no paralysis was employed and 5 when no premedication was used at all. The rate of bradycardic events was less in the paralytic group but rates of oxygen desaturation between the three arms were no different.
Paralysis does make a difference in reducing the incidence of such events and moreover when only looking at the rate of severe adverse events as defined above the finding was that none occurred when paralysis was used vs 9 when no paralysis was employed and 5 when no premedication was used at all. The rate of bradycardic events was less in the paralytic group but rates of oxygen desaturation between the three arms were no different.
 I thought it would be appropriate to provide a few comments on this topic.
I thought it would be appropriate to provide a few comments on this topic.
 I missed him on my last trip to Stockholm as I couldn’t make it to Karolinska University but we managed to meet each other in the end. As we caught up and he learned that I operated this site he passed along a paper of his that left an impact on me and I thought I would share with you.
I missed him on my last trip to Stockholm as I couldn’t make it to Karolinska University but we managed to meet each other in the end. As we caught up and he learned that I operated this site he passed along a paper of his that left an impact on me and I thought I would share with you.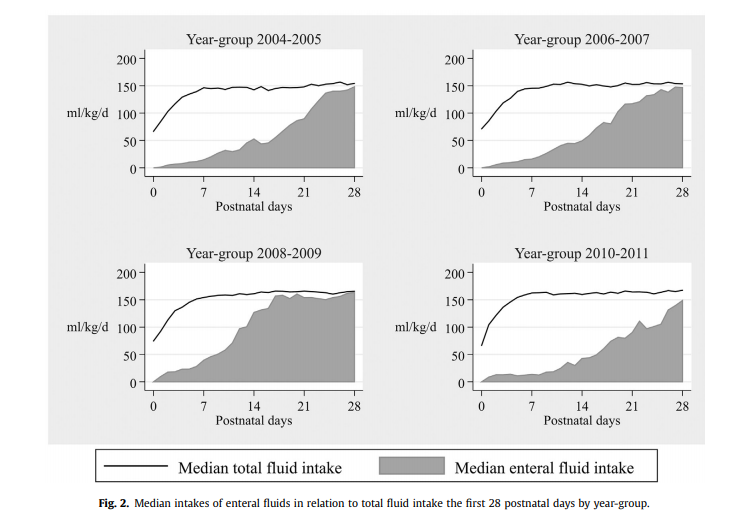


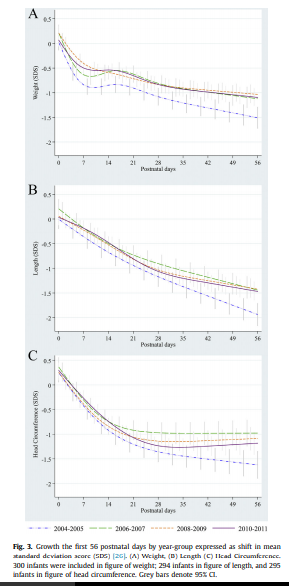 period there were declines in growth across all three measurements compared to expected growth patterns, when one compares the first epoch in 2004-2005 with the last 2010-11 there were significant protective effects of the nutritional strategy in place. The anticipated growth used as a standard was based on the Fenton growth curves.
period there were declines in growth across all three measurements compared to expected growth patterns, when one compares the first epoch in 2004-2005 with the last 2010-11 there were significant protective effects of the nutritional strategy in place. The anticipated growth used as a standard was based on the Fenton growth curves.