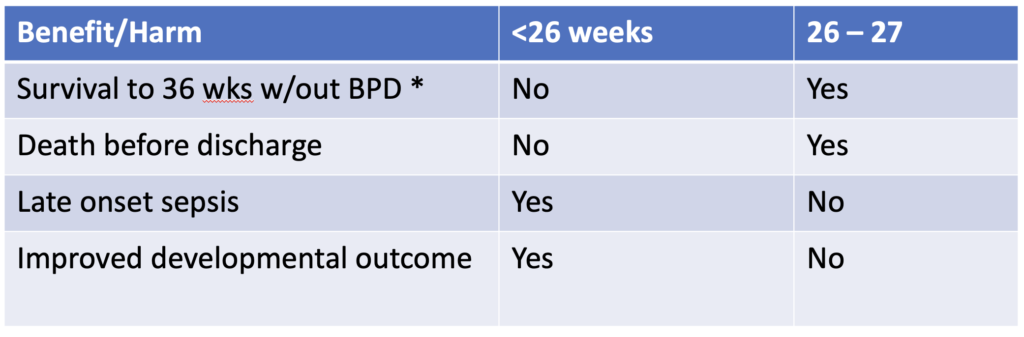
Precision medicine is a growing field in which genetic factors, environment, metabolism and even lifestyle are taken into account when deciding who should receive a treatment or not. When it comes to bronchopulmonary dysplasia I believe anyone who works in Neonatal care can attest it is a mystery why some infants go on to develop BPD while others don’t. We do know that certain treatment strategies may increase risk such as using excessive volumes or pressure to ventilate and in the last 25 years the notion that your level of cortisol in the blood may make a difference as well. I have written about prophylactic hydrocortisone use before in Hydrocortisone after birth may benefit the smallest preemies the most! When looking at the literature thus far and taking into account the results of the individual patient meta-analysis the following table can be generated highlighting a summary of benefits.
The question thus becomes if there is benefit for some infants under 26 weeks and then for some that are 26 and 27 weeks but there is also risk of harm, is there a way to select out those who are most likely to benefit with the least risk of harm.
A baby’s initial cortisol level may be the answer
The PREMILOC study was a double-blond multicentred trial of 523 infants randomly assigned to either prophylactic hydrocortisone in the first 24 hours of life or placebo. All infants were under 28 weeks at birth and received 1 mg/kg/d of hydrocortisone 1 mg/kg/d for 7 days followed by 3 days of 0.5 mg/kg/d for three days. In a pre-planned study coming out of the PREMILOC study, researchers looked at the role of baseline cortisol in predicting response to treatment or risk of adverse outcomes.
What they found in examining baseline levels for both treatment and placebo groups was that a relationship exists between the baseline level and such outcomes.
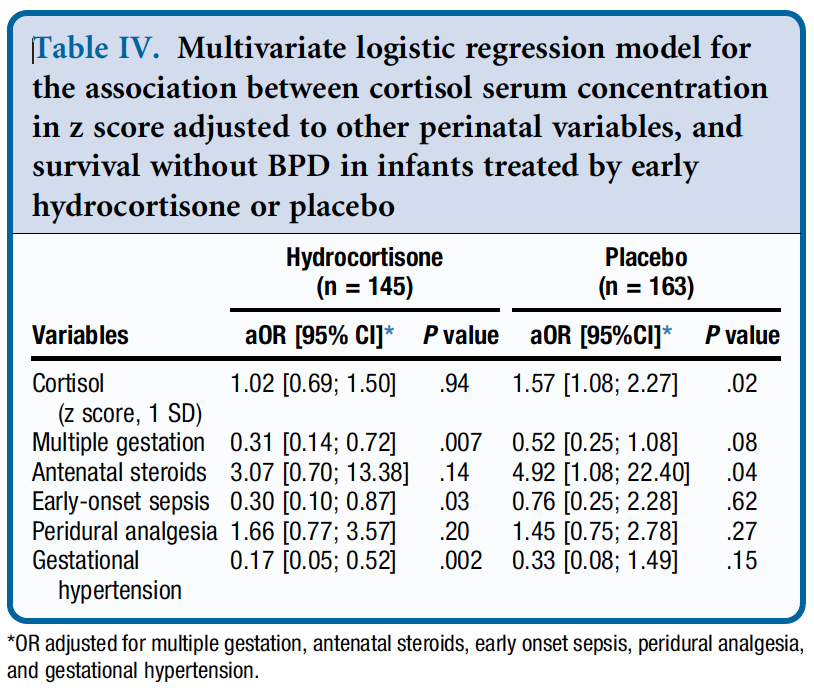
From Table 4 they found a relationship between survival without BPD and a higher initial level of cortisol but found no such relationship in the treatment arm. The threshold of what was considered high was 880 nmol/L although the mean cortisol was in the 400-500 nmol/L range. in other words, if having adequate physiologic levels of cortisol is the goal and a baby already has that, giving more non-antiinflammatory dosing of hydrocortisone doesn’t yield benefit.
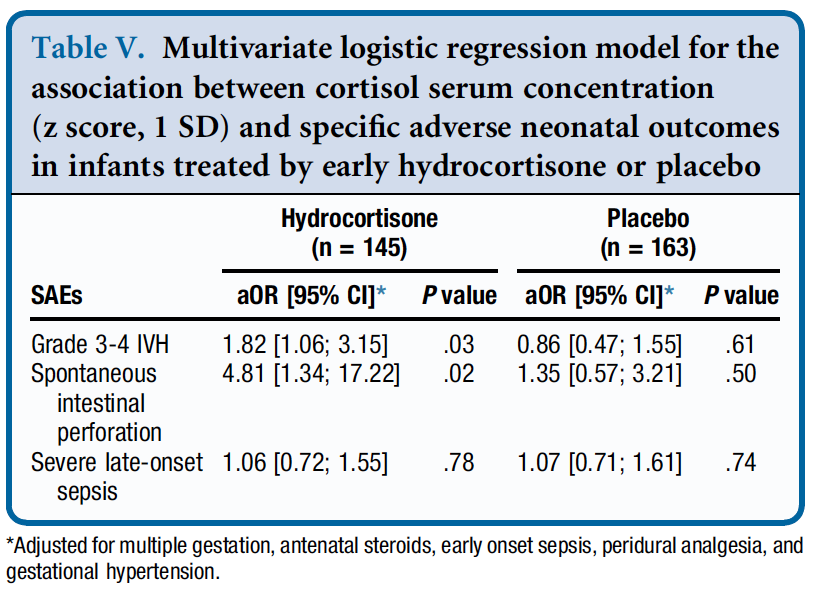
Similarly, when looking at side effects a positive correlation was found between higher baseline levels of cortisol and risk of grade III/IV IVH and spontaneous intestinal perforation. It would seem therefore that if a baby has the level of cortisol that they would normally have from a physiologic perspective they are no different than a placebo arm patient when given hydrocortisone as you bring them to where they need to be. When you double the dose however that they should have, side effects begin to rear their ugly head.
How can you use this information?
From personal conversations I know that many centres are struggling with what to do about giving hydrocortisone. On the one hand there isn’t much benefit (if at all) for BPD in the 24 and 25 week infants but they do better from a neurodevelopmental standpoint. On the other hand there is a benefit in the 26 and 27 week infants but you may predispose them to side effects as well.
This is where precision medicine comes in. One option for centers unsure of who to provide this to (if at all) could be to use a threshold of 880 nmol/L and if the initial level is above this you would not treat but if below offer treatment. This level while found in the study to be predictive of side effects in particular if high does seem very high to me. I would think most babies would qualify which is not necessarily a bad thing but in our center we have typically used levels above 400 or 500 as an adequate stress response. Regardless of the level picked one would be using physiologic data to determine who to give hydrocortisone to as a way to try and maximize benefit and minimize harm for the individual patient.
Make no mistake. Regardless of whether you decide to try this for your patients I don’t believe this is a magic bullet. The best chances for our patients come from having bundles of evidence based based practices and applying them to the patient population if we hope to reduce BPD and minimize risk from any side effects of our treatments. The question is whether prophylactic hydrocortisone should be part of this bundle.
One of the benefits of operating this site is that I often learn from the people reading these posts as they share their perspectives. On a recent trip I was reunited with Boubou Halberg a Neonatologist from Sweden whom I hadn’t seen in many years. I missed him on my last trip to Stockholm as I couldn’t make it to Karolinska University but we managed to meet each other in the end. As we caught up and he learned that I operated this site he passed along a paper of his that left an impact on me and I thought I would share with you.
When we think about treating an infant with a medicinal product, we often think about getting the right drug, right dose and right administration (IV, IM or oral) for maximum benefit to the patient. When it comes to nutrition we have certainly come a long way and have come to rely on registered dietitians where I work to handle a lot of the planning when it comes to getting the right prescription for our patients. We seem comfortable though making some assumptions when it comes to nutrition that we would never make with respect to their drug counterparts. More on that later…
A Swedish Journey to Ponder
Westin R and colleagues (one of whom is my above acquaintance) published a seven year retrospective nutritional journey in 2017 from Stockholm entitled Improved nutrition for extremely preterm infants: A population based observational study. After recognizing that over this seven year period they had made some significant changes to the way they approached nutrition, they chose to see what effect this had on growth of their infants from 22 0/7 to 26 6/7 weeks over this time by examining four epochs (2004-5, 2006-7, 2008-9 and 2010-11. What were these changes? They are summarized beautifully in the following figure.
Not included in the figure was a progressive change as well to a more aggressive position of early nutrition in the first few days of life using higher protein, fat and calories as well as changes to the type of lipid provided being initially soy based and then changing to one primarily derived from olive oil. Protein targets in the first days to weeks climbed from the low 2s to the mid 3s in gram/kg/d while provision of lipid as an example doubled from the first epoch to the last ending with a median lipid provision in the first three days of just over 2 g/kg/d.
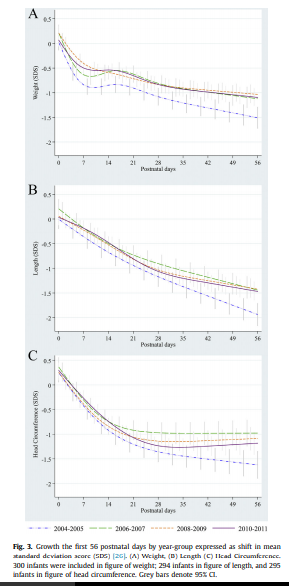
While figure 3 from the paper demonstrates that regardless of time period there were declines in growth across all three measurements compared to expected growth patterns, when one compares the first epoch in 2004-2005 with the last 2010-11 there were significant protective effects of the nutritional strategy in place. The anticipated growth used as a standard was based on the Fenton growth curves.
What this tells us of course is that we have improved but still have work to do. Some of the nutritional sources as well were donor breast milk and based on comments coming back from this years Pediatric Academic Society meeting we may need to improve how that is prepared as growth failure is being noted in babies who are receiving donated rather than fresh mother’s own milk. I suspect there will be more on that as time goes by.
Knowing where you started is likely critical!
One advantage they have in Sweden is that they know what is actually in the breast milk they provide. Since 1998 the babies represented in this paper have had their nutritional support directed by analyzing what is in the milk provided by an analyzer. Knowing the caloric density and content of protein, carbohydrates and fats goes a long way to providing a nutritional prescription for individual infants. This is very much personalized medicine and it would appear the Swedes are ahead of the curve when it comes to this. in our units we have long assumed a caloric density of about 68 cal/100mL. What if a mother is producing milk akin to “skim milk” while another is producing a “milkshake”. This likely explains why some babies despite us being told they should be getting enough calories just seem to fail to thrive. I can only speculate what the growth curves shown above would look like if we did the same study in units that actually take a best guess as to the nutritional content of the milk they provide.
This paper gives me hope that when it comes to nutrition we are indeed moving in the right direction as most units become more aggressive with time. What we need to do though is think about nutrition no different than writing prescriptions for the drugs we use and use as much information as we can to get the dosing right for the individual patient!
I know it sounds absurd that the President of the United States of America should listen to two Hollywood actors but there may be something to this title. In 1997, a movie starring the two actors named Gattaca was released. The premise of the movie was that sometime in the future we would be able to sequence the genes of all humans. Having this knowledge would allow society to direct people towards certain paths in life. Imagine you carried a genetic marker associated with above average mathematical and visual spatial skills. Your parents would be told after analyzing just one drop of blood that you would best be suited to becoming an architect or engineer; two professions where this enhanced skill set would confer an advantage. I have to admit the movie captivated me as a young medical student and I dreamed of such applications in the future as in the “real world” gene sequencing was an ever growing reality.
The human genome has been mapped. As the science of genomics moves along the identification of more and more mutations in genes that either increase the risk of one developing a condition or be born with one are increasing. As an example, a specific mutation that leads to cystic fibrosis can be identified prenatally and prophylactic treatment started soon after birth to modify the course of the condition. This is an example of a screening test and by definition the purpose of screening for conditions is that by knowing the condition exists one can do something about it. This is the justification for newborn screening programs across Canada and the US and has been successful in preventing adverse outcomes for such conditions as phenylketonuria, galactosemia, hypothyroidism and many other diseases as well. These tests are not genetic based but rather look for metabolites in the blood that are elevated due to an error in the metabolism of some enzyme, hormone or other molecule in the body. The establishment of widespread screening programs is a success in modern medicine and one to be celebrated.
What about the field of Genomics then which involves the mapping of human genomes? If using a metabolite that is elevated to identify a condition is possible why not go further and identify causative genetic mutations? The answer lies in something that has been called “Precision Medicine”. This is where President Obama comes in. While Governor of Illinois he first put his weight behind the concept by drafting a bill that was not passed but endorsed by his office nonetheless. Now we come to 2015 and as President he has again raised the need for funding of such work by asking congress for $215 million dollars to fund the “Precision Medicine Project” which was announced in January 2015.
The goal of the project is to sequence the DNA of both healthy and ill individuals and identify genetic determinants of health. In fact pilot projects are already underway in some centres in the US and in this case are studying infants including 400 at the University of North Carolina Chapel Hill. Does this sound like a certain movie to you?
Before you think that I am against such advancement in medicine I am all for it but with some words of warning. We have known for some time that many types of cancer are caused by different genetic mutations that cause cells to start growing into tumours or abnormal cells in the case of leukemia. Knowing these genetic markers allows Oncologists to choose the right chemotherapy or other treatment to offer you the best chance of survival. Similarly as Angelina Jolie found, having the BRAC1 gene influenced her decision to have her ovaries removed after her double mastectomy before they could develop cancer. Having this information allows the individual to make an informed decision as to what is in the best interests for themselves and their loved ones.
Why is any of this concerning?
The issue though in all of this centres around several very concerning points. What happens to these blood spots that a nurse collects after doing the routine newborn screening in the hospital. Are they your property, the hospitals or the governments? This is the exact question that culminated in lawsuits in Minnesota and Texas recently. Unbeknownst to parents, their newborn’s blood was being sent to the US Armed Forces DNA Identification Laboratory for the creation of a forensics database. In many other states the blood was being kept for many years without parent’s knowledge. Moreover what would the government do with such data is not clear. The central question then is who has the rights to your babies DNA? For a more in-depth analysis of the history and the legal issues please read this http://www.usnews.com/opinion/articles/2014/04/28/newborn-screenings-violate-dna-privacy-rights
The second issue on the horizon has to do with the concept of a screening test. As mentioned before the purpose of screening programs are to identify treatable conditions early, such that preventative medicine to avoid complications can be started. As medicine moves along and identifies thousands upon thousands of causative genetic mutations there is a tremendous risk of straying from the intent of screening and moving towards simply identifying conditions that may not be treatable or may not affect an individual until adulthood. Take for example that a newborn screen identifies that your child is at high risk of developing early onset coronary artery disease 30 – 40 years from now. What if they are predicted to develop glaucoma in their 30s? You could go on and on with these examples but what impact could that have on their life. As a parent would you encourage them to become an elite athlete knowing they could have a myocardial infarction from coronary ischemia in their 30s? Would you support them in becoming an Ophthalmologist when you knew they were likely to develop glaucoma and visual disturbance early in their career making it difficult for them to practice? Would it have been better to not know and let them pursue their dreams even if only for a limited time? Taken to the extreme if you knew they carried a mutation leading to an untreatable condition that leads to death in their 30s ninety percent of the time what type of quality of life would they have?
The last point has to do with who owns the information. If it is indeed the government then could a world as portrayed in Gattaca not be that far off. Could parents be told soon after birth that their child will not be eligible for certain occupations or directed into specific paths? Could future employers request this information as part of a disclosure for being considered for a job? In the 90s we saw such fear become a reality when many individuals refused to have HIV testing as they were concerned the test alone would make them ineligible for life insurance.
Lastly could we see a world in which many births would never happen as prenatal testing might identify conditions that the fetus would one day develop as adults and parents decide that the child’s life was not worth living?
I don’t think Gattaca has arrived…yet. The point of all of this is that we need to tread the field of genomics very carefully. Medicine has a long history of developing technology that had the greatest promise and then once in use raised the classic question “Just because we can do this should we?” I sincerely hope that President Obama and the rest of the developed world consider these issues as we move forward which I am sure we will. We are on the cusp of a dramatic shift in the way medicine in practiced. Precision Medicine is upon and if you think that I am talking about something that is off in the distant future please look at these hospital websites where you can have your “Precision Medicine” already. I wonder what Uma Thurman and Ethan Hawke think about all of this?



 I missed him on my last trip to Stockholm as I couldn’t make it to Karolinska University but we managed to meet each other in the end. As we caught up and he learned that I operated this site he passed along a paper of his that left an impact on me and I thought I would share with you.
I missed him on my last trip to Stockholm as I couldn’t make it to Karolinska University but we managed to meet each other in the end. As we caught up and he learned that I operated this site he passed along a paper of his that left an impact on me and I thought I would share with you.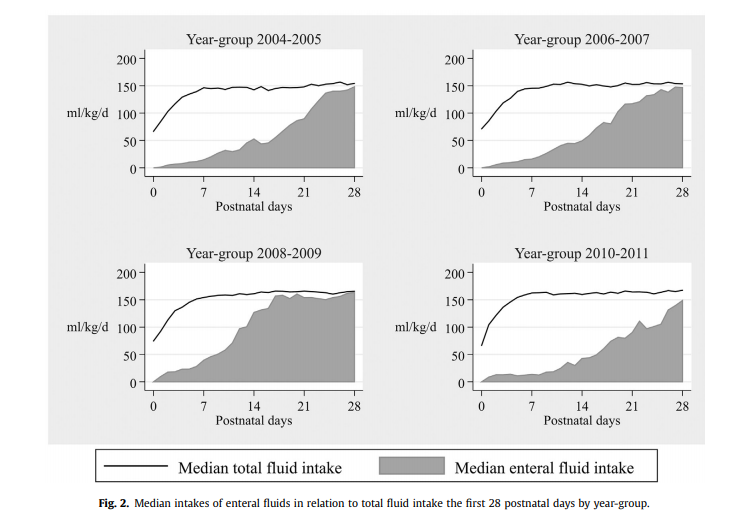


 period there were declines in growth across all three measurements compared to expected growth patterns, when one compares the first epoch in 2004-2005 with the last 2010-11 there were significant protective effects of the nutritional strategy in place. The anticipated growth used as a standard was based on the Fenton growth curves.
period there were declines in growth across all three measurements compared to expected growth patterns, when one compares the first epoch in 2004-2005 with the last 2010-11 there were significant protective effects of the nutritional strategy in place. The anticipated growth used as a standard was based on the Fenton growth curves.