Anyone who works in the NICU is more than familiar with the sad moment when you find out an infant has suffered a severe IVH (either grade III or IV) and the disclosure to the family. The family is in a state of shock with the fear of ventricular drainage a reality that will likely come to pass. We have spent many years trying to find ways to reduce this risk and antenatal steroids and delayed cord clamping are two relatively recent interventions that have had a real impact. Unfortunately we have not been able to eliminate this problem though. What if something as simple as an exclusive human milk diet could be that magic bullet to further reduce this problem in our NICUs?
Exclusive human milk diets
I have written about this topic before but as a refresher this generally refers to all sources of nutrition being derived from human milk. Ideally we would provide mothers own milk (MOM) but when this is not available units rely on pasteurized donor human milk (PDHM) as the base feed. Added to this is human derived human milk fortifier (H2HMF) as opposed to bovine powdered or liquid fortifier usually to provide a base caloric density of 24 cal/oz.
Reducing IVH Through Exclusive Human Milk Diets
It would be nice to have a prospective multicentre trial with this as the outcome but there is a significant problem when doing this type of study. The H2HMF is costly with a price tag of about $13-15000 per treatment course so to do a prospective RCT would not be easy for units that don’t use the product already. Moreover, for those units that are already sold on the product it would seem unethical if there was no equipoise to randomize to bovine or human fortifier. As such, when we talk about getting the best evidence it is most likely going to come in the form of a retrospective study as has been done here by Carome K et al in their paper Exclusive human milk diet reduces incidence of severe intraventricular hemorrhage in extremely low birth weight infants.
The authors in this study chose to look at three different time periods with different approaches to feeding of ELBW infants. They were as follows with all diets providing H2HMF going until 34 weeks. Aside from the source of nutrition, starting of and incremental advancement of feedings was protocolized as per unit approach.
2012 to 2014 – MOM was given when available. Preterm formula was the alternative as a supplement Fortification of was with bovine milk-derived liquid fortifier 2014 to 2015 – H2HMF used in those infants receiving exclusively MOM. All others received preterm formula as supplement or alternative. If MOM was available but in insufficient quantities for sole diet, it was fortified with bovine-HMF 2015 to 2017 – all ELBW infants received an EHM diet consisting of MOM if available and PDHM as a supplement to MOM or as full diet, each fortified with H2HMF
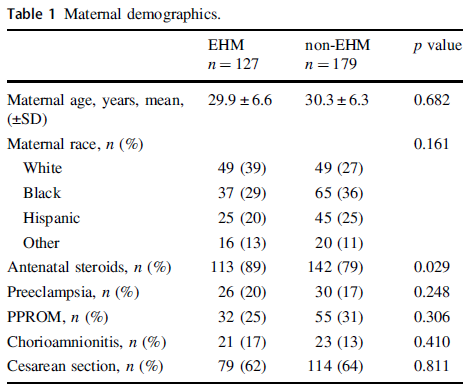
The maternal demographics were similar between those receiving exclusive human milk diets and those without except for a higher antenatal steroid provision in the EHM group. This of course bears consideration in the results as steroids have been shown to reduce IVH.
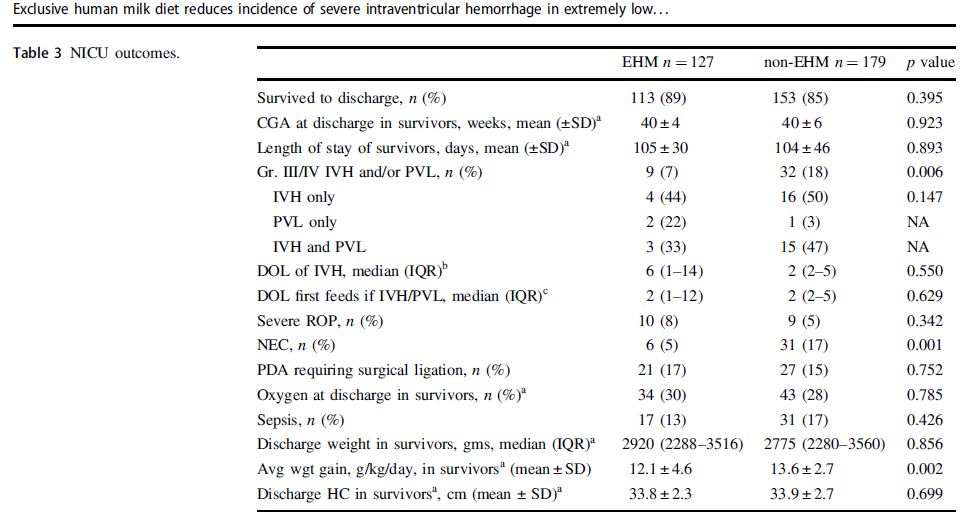
Looking at the results below shows some very promising findings. The incidence of Grade III/IV IVH and/or PVL was 7% in the EHM group and 18% in the non-EHM group. Also noted to be quite different was the incidence of NEC which was 5% in the EHM and 17% in the non group. The authors also did a subgroup analysis looking at the use of MOM vs PDHM and found no difference in outcomes regardless of source of human milk used. As the authors point out this might mean that the pasteurization process does not denature the components of milk responsible for these protective effects if the results are to be believed.
One strength of the study was that the authors performed a logistic regression to control for the higher rate of antenatal steroid use and lower rates of NEC in the EHM group since both would be expected to influence rates of IVH/PVL and found that the results remained significant after this analysis. The findings were an OR of 2.7 CI 1.2–6.0, p = 0.012 so that is promising!
What They Weren’t Able to Do
It’s possible I missed it in the article but like several other papers on this topic the babies who received formula and those who received human milk with bovine fortifier were grouped together. As such what we don’t know from this study is whether the addition of just the bovine fortifier vs H2HMF would have yielded the same results.
Nonetheless what the article does suggest is that use of EHM diets are protective against severe IVH/PVL regardless of the source of human milk when you compare it to receipt of any bovine sources. The caveats about retrospective studies of course exist as per usual but if this is the best evidence we have how do we use it? At the very least this calls out for strategies to maximize milk production for mothers and to use PDHM when MOM is not available. It certainly is suggestive that the use of H2HMF may confer benefit as well. What you unit does with this information I suppose will need to be determined based on the totality of the evidence. I suspect there is more of this story to be told and this adds yet another chapter in the tale of EHM.
Phenobarbital at least where I work has been first line treatment for seizure control for as long as I can recall. We dabbled with using phenytoin and fos-phenytoin in the past but the go to tried and true has been phenobarbital for some time. The use of this drug though has not been without trepidation. Animal studies have linked phenobarbital to increases rates of cerebral apoptosis. Additionally, in a retrospective comparison of outcomes between seizures controlled with phenobarbital vs Levetiracetam, the latter came out ahead in terms of better long term developmental outcomes. This study from 2013 was entitled Adverse neurodevelopmental outcomes after exposure to phenobarbital and levetiracetam for the treatment of neonatal seizures. Purists of course would argue the need for a prospective trial and that is what we have to chat about here.
Levetiracetam vs Phenobarbital
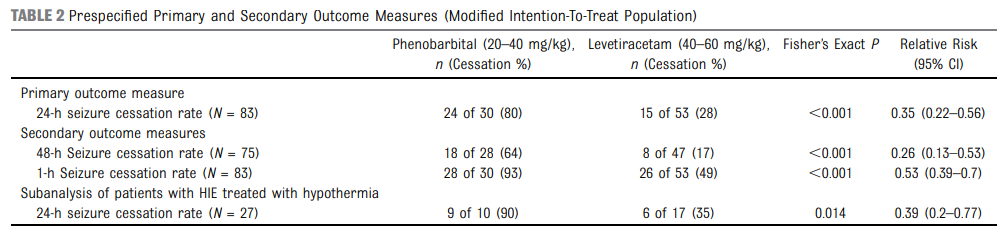
The study in question was a multicenter randomized phase IIb trial (searches for a dose that provides biological activity with the minimal side effect profile) that compared two doses 40 mg/kg and 60 mg/kg of Levetiracetam with standard doses of phenobarbital. The study was done by Sharpe C et al and called Levetiracetam Versus Phenobarbital for Neonatal Seizures: A Randomized Controlled Trial.
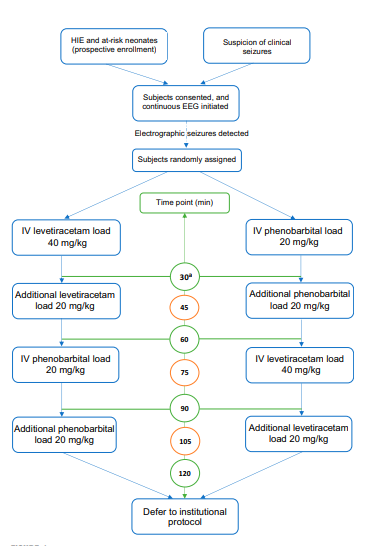
In this study patients were randomized to receive levetiracetam or control phenobarbital treatment group in a 60:40 allocation ratio by using a block randomization strategy and stratified by site. The trial design is shown in the diagram below.
The study was designed to not delay institution of the accepted treatement with phenobarbital as usual first line treatment of seizures by more than 1 hour. The strength of this study was that the authors used electrographic seizures confirmed by continuous EEG monitoring. The efficacy of medication effect was blindly interpretted by two independent electrophysiologists. in other words the authors went out of their way to ensure these were real seizures and moreover that any changes to medications were decided upon after interpretation of effect by people remote from the study. The primary outcome though in comparison to the aforementioned retrospective study was a short one. In this study the primary outcome was initialy absense of seizures for 48 hours but then was changed part way through the study to 24 hours. The change was a practical one since it was noted after data collection that in many cases EEG monitoring had been stopped prior to 48 hours.
The Results
Honestly it is the results that led me to want to talk about this study. They are the exact opposite of what i thought they would be. Based on my own experience with Levitiracetam seeming like a wonder drug when it comes to seizure control I expected the results to favour it. Not the case.
To say that phenobarbital crushed the competition is an udnerstatement. Having said that the incidence of side effects were higher with phenobarbital as well. Hypotension, respiratory suppression, sedation, and requirement for pressor support, were more common. Nonetheless, this study also included patients with HIE and found even in this subgroup phenobarbital was superior. This is important information as one could speculate that earlier seizure cessation in those with anoxic injury already could be especially beneficial.
What do we do with these results?
As the authors point out this is a study of short term outcomes. In the trial about long term outcome it was clear that treatment with phenobarbital leads to worse outcome than with levitiracetam. Having said that it was a retrospective study so the next step will be to conduct long term outcome studies to see effects. This presents the possibility of an interesting conundrum. What if the newer drug is inferior to tried and true phenobarbital at controlling seizures but leads to better long term outcome? Would you consider allowing seizures to persist longer than you might otherwise want to in the short term but then be able to reassure families that the long term outlook is bettter? The side effect profile of levitiracetam is such that I think neurologists want to use it but the other possibility is that there is another newer anticonvulsant that will need to be tested as wouldn’t it be great not to have to choose either poor acute seizure control but better long term outcome vs better seizure control with concerning long term outcome? As a parent I have no doubt watching a child eize would be terrifying and you would want it to end as soon as possible but the question with phenobarbital is at what cost?
The infant car seat challenge(ICSC) is a test which most definitely fits the definition of a battleground issue in Neonatology. After publishing the Canadian Pediatric Practice point on the same topic I received interesting feedback through the various social media forums that I frequent. While some were celebrating the consensus of the statement as verification that a centres’ non practice of the test was acceptable, others seriously questioned the validity of the position. The naysayers would point out that extremely infrequent events unless intentionally tracked may be difficult to pick up. In the case of the ICSC, if a few patients were to suffer a hypoxic event leading to an ALTE or worse after discharge, could the ICSC have picked out these babies and prevented the outcome? The evidence for adverse events associated with the use of car seats as discussed in the position statement is poor when using autopsy records over decades but when many clinicians can point to a failed ICSC picking up events, the thought goes that they “caught one”. Does catching one make a difference though?
The Well Appearing Infant
Shah et al in their recent paper Clinical Outcomes Associated with a Failed Infant Car Seat Challenge attempt to address this very point. They performed a retrospective study of 148 patients who were either <37 weeks GA or < 2500g at birth. The study was made possible by the fact that all such infants in their hospital admitted to a well newborn area meeting these criteria by policy must have an ICSC prior to discharge. Keep in mind that these were all infants who were on the well newborn service since they were asymptomatic. The definition of an event in this group was one or more of pulse oximeter saturation ≤ 85% for > 10 seconds, apnea > 20 seconds, bradycardia < 80 bpm for > 10 seconds, or an apnea or bradycardia event requiring stimulation. The failure rate was 4.5% which is very similar to other reported studies.
Why did they “fail”?
Failure of the ICSC was owing to desaturation 59%
Bradycardia 37%
Tachypnea 4%
Combination of 2 in 11%
What is interesting about these results is what happened to these infants after admission to the NICU in that 39% were identified with apnea (48% in preterm vs 17% in term infants). These events were in the supine position which is a curious finding since the ICSC was designed to find risk of cardiorespiratory stability in a semi-recumbent position. This has been shown previously though.
What does it all mean?
The infants in this study ultimately had more NG feeding, prolonged length of stay and septic workups after failing the ICSC that comparable infants who passed. At first blush one would read this article and immediately question the validity of the CPS position but then the real question is what has this added to the “pool of knowledge”. That infants may fail an ICSC at a rate of 4.5% is already known. That such infants may demonstrate apneic events has also been shown before and a study like this may help to support those clinicians who feel it is still imperative to find these infants in order to achieve a safe discharge. I think it is important to put these findings in the context of what would have happened if such a unit did not routinely test these types of babies. As all were seemingly well and I presume feeding with their families, they would have been discharged after 24-48 hours to home. We have no evidence (since they have not compared this sample to a group who did not have such testing) that if these babies were discharged they would have faired poorly.
The supporters of the ICSC would point to all the support these babies received by admitting them for 6-8 days, providing NG feeding and ruling out sepsis that they were unsafe for discharge. The other possible way to look at it was that the infants were subjected to interventions that we have no evidence helped them. Whether any of these infants had a positive blood culture justifying antibiotics or needed methylxanthine support is not mentioned. Judging however by the short length of stay I suspect that none or few of these infants needed such medication as I would expect they would have stayed much longer had they needed medical treatment for apnea.
Conclusion
I do commend the authors for completing the study and while it does raise some eyebrows, I don’t see it changing at least my position on the ICSC. While they have described a cohort of patients who failed the ICSC nicely, the fundamental question has been left unanswered. Does any of this matter? If you look well, are feeding well and free of any clinically recognizable events but are late preterm or IUGR can the ICSC prevent harm? This has not been answered here and perhaps the next step would be for a centre that has abandoned the ICSC to follow their patients after discharge prospectively and see whether any adverse outcomes do indeed occur. Any takers?
I suppose I am as guilty as anyone with respect to the evolution of this story. Twenty years ago early and late cranial ultrasounds were employed to give clinicians some guidance as to what to tell parents about their growing preterm infant. Blood seen on early ultrasounds might influence aggressiveness of care or help us remain vigilant for the development of evolving hydrocephalus. Similarly, late cranial ultrasounds might detect periventricular leukomalacia or other white matter injury and alert us to a higher risk of cerebral palsy. Then things changed with the widespread availability of MRI. As I have mentioned to countless parents, MRI compared to ultrasound is like comparing an old 1 megapixel camera to a modern day 18 megapixel. The resolution is simply much better and with it our ability to see things that previously escaped our detection.
As utilization of MRI increased so did publications pertaining to its findings. With the enhanced clarity, white matter lesions that were previously missed became evident and imaging of the posterior fossa or specifically the cerebellum improved as described by Tam et al. Bleeds in this area that were previously missed could now be readily seen, although more recently use of the mastoid view when performing cranial ultrasound may pick up many significant lesions as well. Fear in the medical community arose in 2007 after a paper entitled Does Cerebellar Injury in Premature Infants Contribute to the High Prevalence of Long-term Cognitive, Learning and Behavioral Disability in Survivors by Limperopoulos et al. In this study of 86 patients overall, presence of cerebellar injury with or without supretentorial lesions was associated with neurodevelopmental impairment in 66% versus 5% of age matched controls. Given that cranial ultrasound may miss such cerebellar lesions it seemed prudent to begin imaging all high risk patients at term to determine if there was a significant risk of long-term disability. As Neonatologists we are often asked if a families baby will be ok and so with the ability to obtain such information why would one not pursue such imaging?
With this finding, utlilization of MRI at term equivalent age became widespread including our own centre. In hindsight however this practice was not thought out carefully and the ramifications of this decision were significant. One of the most common things that we teach to medical students is the practice to ask themselves the following question before they do any diagnostic test.
“How will the results of this test influence your management?”
If the result is positive what will you do and similarly if it is negative will this help you in any way. It is the answers to these questions that leave me with a desire to travel back in time and influence my colleagues to choose a different path than we did. The problem lies in the meaning of the test, either positive or negative and what if anything we will do with the result that is different than if we had not known in the first place. This issue was recently highlighted in a large trial from the NICHD entitled Neuroimaging and Neurodevelopmental Outcome in Preterm Infants. The results of the MRI studies compared with cranial ultrasound demonstrated again the superior capabilities of MRI to diagnose cerebellar bleeds but as can be seen in the following table, the absence of any lesions on MRI does not mean the parents should be told all will be well with their infant.
Severity of WMA
Normal
Mild
Moderate
Severe
Cognitive score < 70
4.1
4.3
10.5
22.2
Corgnitive score < 85
20.4
18.2
29.9
61.1
Any CP
2
5.4
5.9
61.1
Moderate to severe CP
0
1.9
1.5
55.6
NDI
4.1
6.2
10.5
55.6
From the table you will note though that with increasing injury, the risk of adverse outcomes increase as well. On the surface this would imply that the information may be important, as we may be able to tell the parents that we are concerned if the lesions are more significant. What would we do with this information though that is not already being done? Herein lies the major issue in all of this.
Modern NICU care entails having a follow-up program for all patients designated as high risk. In the case of our centre this means having a multidisciplinary team evaluating all infants born under 1500 g. Infants who in follow-up demonstrate deficits whether they be cognitive, motor or both are provided with the support they need to address these deficits. Whether the family knows that there is an abnormality in the MRI or not does not influence the trajectory they are on in terms of evaluation and suggestions for any therapies that are needed. The use of the MRI fails the test that I mentioned earlier. If it is normal the child may still have deficits or if abnormal the infant could still be unimpaired. The fact that the degree of severity on the MRI being more predictive of an abnormal outcome does nothing more than provide families with something to worry about pending the formal testing when they are seen in follow-up.
You may think I am being paternalistic to a certain degree but these beliefs were illustrated by a family after their experience at St. Justine in Montreal. I suspect that the practice has changed there but at the time as was done in Winnipeg, MRIs were done at term equivalent age for all infants under a certain weight. The case of Maren, a surviving twin, born at 25 weeks gestational age was one in which she was diagnosed with a cerebellar hemorrhage on MRI. The family took to the internet as many parents do and uncovered the paper on cerebellar bleeds referenced above and spent the next several months in anguish as they waiting for the results of the follow-up testing and moreover seeing how she would develop. I think this quote from the article sums it up very well as to what the test meant for them.
“In our case, Maren’s MRI gave us no information about what she is like today, it served only to completely terrify us. Maren is now two and a half with no disabilities”
This past month the AAP released a “Choosing Wisely” recommendation on this practice and suggests as I have that it be stopped. I hope for the sake of families everywhere this is widely adopted. Sometimes it is just better to leave things well enough alone when all that your test will do is create more anxiety for parents who have already experienced enough.
Those are the first words that a parent given the diagnosis of stroke says after hearing the news. It is perhaps one of the worst nightmares a new parent can have. A baby is carried to full term and is born after a seemingly uneventful delivery with normal apgar scores. The family spends the first day together getting to know each other and planning for life outside the hospital. Then sometime between the first and third day of life the parents note their infant shaking an arm or leg repeatedly and call the nurse for assistance. A physician arrives and informs the parents that she believes their newborn is having a seizure and orders phenobarbital, which the parents have never heard of. Shortly afterwards, the family is told that their child needs an MRI and an hour later when the report comes in their world is shattered as they are informed that their infant has a stroke.
At this point their minds flood with memories of elderly relatives or assisted living homes where they met people with strokes and with that their world and dreams are vanishing in front of their wyes.. Lost is the sense that they will have a normal child when they go home but is this what they should expect or is the experience of the family in the following video what is more likely to occur. Such a story told through the experience of a family in this TED talk so well captures the essence of these feelings that I urge you to watch it before moving on.
Shocking as it may be to hear that a newborn has had a seizure, the reality is that the frequency of such events is no different than in adults. Moreover the newborn period has the highest rate of stroke than any other time in childhood. The overall incidence of neonatal seizures is between 1:2000-3000 live births.
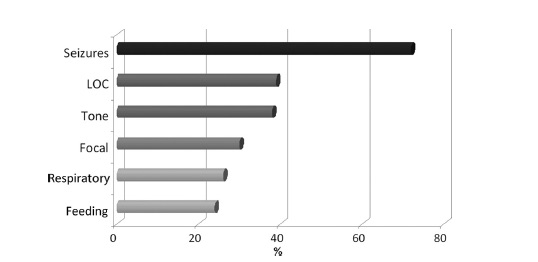
Stroke in a newborn is frightening and from the International Pediatric Stroke Study we have the following figure that provides information as to what these children present with. The symptoms usually present as they did in the case above sometime after 24 hours and consist of the following.
How do they do in the long run?
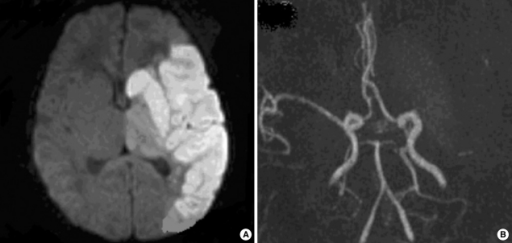
We are fortunate that the group from Hammersmith has been following a group of neonates since their diagnosis of a middle cerebral artery infarction more than 15 years ago and intermittently reported on their neurological outcomes. In the most recent report at age 9 years published in 2008 the results indicated that of the original cohort of 31 patients about 30% had hemiplegia. Interestingly with respect to cognitive outcome the results were just as promising or perhaps even better in that 21/27 assessed at 9 years had normal intelligence. Of the six children who had an IQ below normal, the lower results may have been explained by something other than a neonatal stroke. Two patients were dysmorphic but without a specific diagnosis, one child had autism, one was too shy to be tested so perhaps had normal intelligence and the last child had signs on the original MRI of significant ischemic damage to the brain stem suggesting an additional insult over and above the arterial stroke.
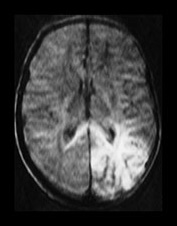
In the Hammersmith cohort almost all patients suffered a left MCA infarct which for reasons that remain unknown is the most common territory affected. The next most common location is the posterior circulation and was the subject of a paper by L de Vries on outcome at a mean age of 36 months.
Out of the 17 patients followed, 5 had a global delay with 9 having visual defects. The presence of visual defects is not surprising given the finding that the infarct in the posterior circulation caused injury to the periventricular white matter. This area of the brain of course is where the optic radiations pass through leading to such a disability. Interestingly only one of the 17 that were followed had a hemiplegia.
As you can see the likelihood in the newborn with a stroke is that they will recover their motor function a great deal and unlike the adult with a similar stroke they are capable of a “rewiring” that provides hope for those parents after the initial devastation of hearing the word “stroke” for the first time.
What features provide a high likelihood of later impairment?
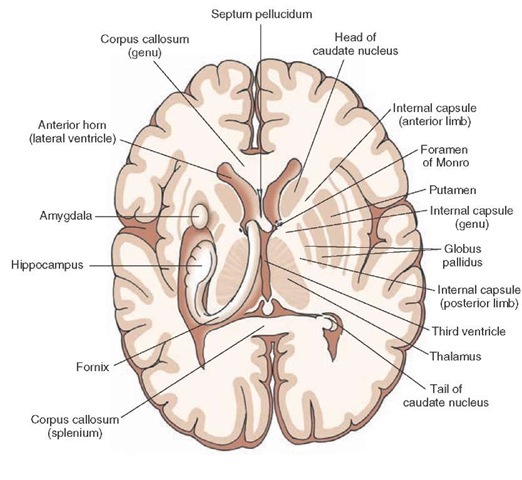
As was shown by Mercuri et al in 1999 the existence of a stroke involving the basal ganglia, internal capsule and hemisphere is predictive of motor impairment. The basal ganglia and other structures mentioned are comprised of several different areas that are labelled in the picture of the brain and are comprised of the putamen, caudate, globus pallidus, the substantia nigra, nucleus accumbens and subthalamic nucleus (the last three not labelled below). Injury to any of these structures along with the internal capsule and other area of the hemisphere would not have a probable good outcome.
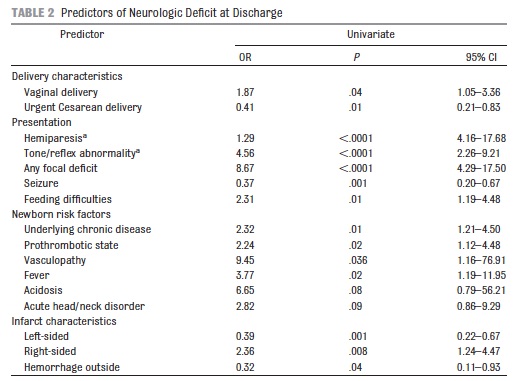
Additional work done by the International Pediatric Stroke Study in 2011 indicated that the following features were predictive of adverse outcome.
It is important to note that this was outcome at discharge for 250 neonates with stroke. It will be interesting to see if the 50% motor impairment at discharge in this cohort diminishes over time as in the Hammersmith group.
So when we look back at the video that is featured in this post I question whether this family was given good information at the outset. Maybe if someone had put together a post like this to share with them (and to put it into slightly more lay terminology) they would have had fear replaced by cautious optimism.
Who knows maybe this post will reach someone and spare them some of the anguish that I imagine this family must have faced?