Jaundice has to be one of the most common issues facing newborns and their families. Whether in the NICU or on the post-partum floor all babies get jaundiced to a certain degree and some become so much so that they require treatment. Many centers the world over have developed home phototherapy programs to allow treatment to be done at home and they are known to be effective. In Sweden such programs exist and in theory sending infants home rather than keeping them in hospital could have positive effects for both the infant and parent dyad in terms of bonding. Keeping the infants in hospital and in particular over the last couple years when in many places of the world COVID protocols made visiting more difficult there is the real potential to disrupt bonding if a baby is otherwise ready for discharge. Researchers in Sweden with such programs in Uppsala recently decided to explore this question about bonding so here we go.
The Study
This was a multicentre study in Sweden by Pettersson M et al entitled Home phototherapy of term neonates improves parental bonding and stress: findings from a randomised controlled trial. The study intended to enroll 250 infant-parent pairs into an RCT comparing in-hospital phototherapy to home phototherapy and determine the status of bonding between child and parents at various time points. The inclusion criteria required infants to be >36 weeks at birth, have non-immune jaundice (DAT -ve) and have a bilirubin at inclusion from 300-400 micromol/L from 48 – 60 hours of age. Infants with asphyxia and weight loss >10% were excluded. Infants were also excluded if their parents did not speak Swedish or if the physician felt they would not be able handle home phototherapy.
In both environments treatment was provided with a biliblanket or overhead blue lights 25 cm from the skin which the infant would lay on or be placed under. These infants did not have severe bilirubin levels so it appears they had only standard phototherapy. This makes sense as babies with higher risk would not be suitable for consideration of home phototherapy.
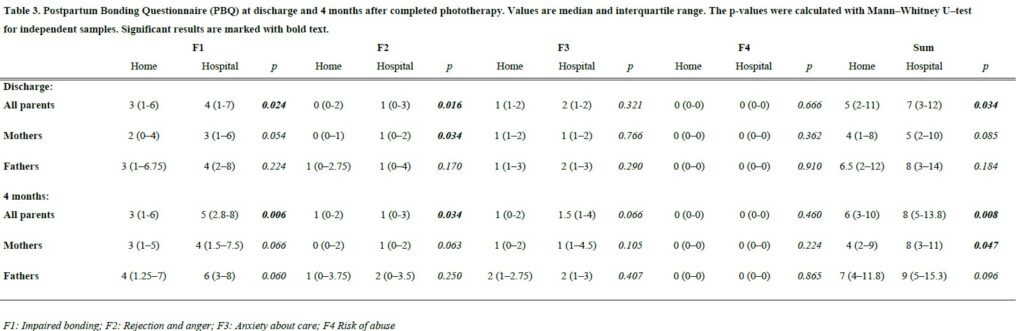
Several validated tools were used to determine such things as bonding, risk of depression and stress. The primary outcome was based on use of the Postpartum Bonding Questionnaire (PBQ). Higher scores indicate worse bonding. The sample size was calculated on results from previous studies showing a mean (SD) of 10.7 (8.5) in 250 newborns with 90% power to detect a three-point difference in mean PBQ-sum for mothers at the 5% significance level, with a pre-planned interim analysis after 125 inclusions.
Enrollment was slow and after the preplanned analysis it was decided to stop the study recruitment and see where the results landed.
The Findings
Both groups of infants were treated for a total of about 4 days with testing for bilirubin levels and treatment with phototherapy (about 18 hours of total treatment both groups). The results of the PBQ found a statistical difference in measures of bonding favouring the home phototherapy group as found in the table below at both discharge and 4 months.
Interestingly when breaking down the results by mothers and fathers there was no impact on bonding for the fathers after this four day period of investigation and treatment at hospital vs in the home but at both time points it was the mother that drove the benefit seen. This likely speaks to differences in the way mothers and fathers experience bonding or perhaps how they process threats to it. No differences in stress could be found between the two groups but it is important to note that the small sample size and the fact that it was a secondary outcome make it difficult to say with certainty that there is no impact on stress.
Thoughts
You would be well within your rights to say “so what? It’s what we expected”. The difference seen in bonding while favouring the at home group has statistical significance but I am not sure to what degree this represents clinical significance. Can you truly perceive a difference in bonding based on a two point difference? Would that be meaningful functionally in the home in the way that parents relate to and respond to their infant? Not sure.
What I think we can say though is that the direction of the effect is certainly positive. We can also say from a systems standpoint that not only is phototherapy using a biliblanket safe and effective but it also moves care to the home and thereby creates room in the hospital for babies who truly need to be admitted.
Given the direction of the effect I think what the study does is provide one more argument aside from improving patient flow to aid in the establishment of home phototherapy programs. There are benefits not only to the family from an earlier discharge but also to some degree improvements in bonding certainly between mother and baby. This brief four day period has impacts that can last all the way out to four months. If you were looking for some evidence to support building such a program, maybe this will help!
If you work in Neonatology then you can’t help but see babies with jaundice. It is so common in the NICU that I would call it normal. While mild jaundice is part of neonatal life, sometimes levels increase to the point that it can be dangerous to the developing brain and in the short term cause acute bilirubin encephalopathy. Chronic injury can lead to hearing impairment and kernicterus with staining of the basal ganglia and cerebral palsy. Phototherapy has been the mainstay of treatment with exchange transfusion reserved for exceptionally high levels of bilirubin. In recent years people have utilized IVIG when hemolysis is present to reduce the risk of exchange transfusion. There hasn’t been much else that one could use but many years ago, proto-porphyrins (SnPP)were looked at as a class of drug that might help reduce the burden of bilirubin by blocking where the substance comes from. Bilirubin is liberated when heme is broken down by heme-oxygenase so an inhibitor of this enzyme (of which the metallo-porphyrins (Sn-MP)might be the right candidate for the job. While initial trials seemed to show benefit there was a side effect of studies in rats indicated that exposure to Sn-PP (but not Sn-MP) led to photosensitivity if exposed to UV light and phototherapy. Given that the Sn-MP class of drugs didn’t seem to have the same issues an interest in this class of drugs has experienced a resurgence.
Phase IIb clinical trial
In the development of drugs there are different phases of trials. In a phase IIb trial, researchers believing from previous research that there is a treatment effect, perform a larger study using different dosing to see if there is still a benefit. In the case of Sn-MP this was done by Rosenfeld WN et al in their recent trial Stannsoporfin with phototherapy to treat hyperbilirubinemia in newborn hemolytic disease. The trial design included infants with hemolytic disease with 91 patients divided into three groups; 31 controls, 30 receiving a 3 mg/kg IM dose and 30 receiving a 4.5 mg/kg IM dose of stannsoporfin along with phototherapy. The goal of the study was to see whether infants receiving such treatments would experience different trajectories in their levels of bilirubin. In order to standardize things as much as possible, all infants were enrolled once they reached a pre-specified level using the AAP phototherapy curves and underwent serial TsB measurements at 2,6,12,24,36 and 48 hours after study entry.
Phototherapy was standardized based on measurement of spectral irradiance at the skin surface with maintenance of 30 microW/cm2/nm to ensure that each infant received the same level of phototherapy.
The Findings
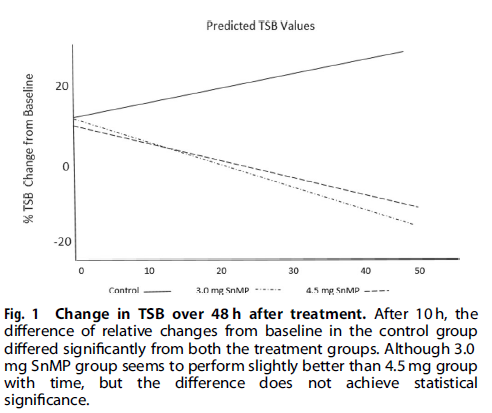
I suppose it shouldn’t shock anyone that the drug works as the class of drug was found to work almost 40 years ago! Looking at the three groups over the 48 hour time frame shows a markedly different trajectory for the patients.
Using an intention to treat analysis the authors noted a 17.5% increase in bilirubin from baseline over 48 hours in the control group and a -13.0 % change in the 3 mg/kg and -10.5% in the 4.5 mg/kg arm. The differences between the two treatment groups compared to the control arm was significant but between the two dosing levels not.
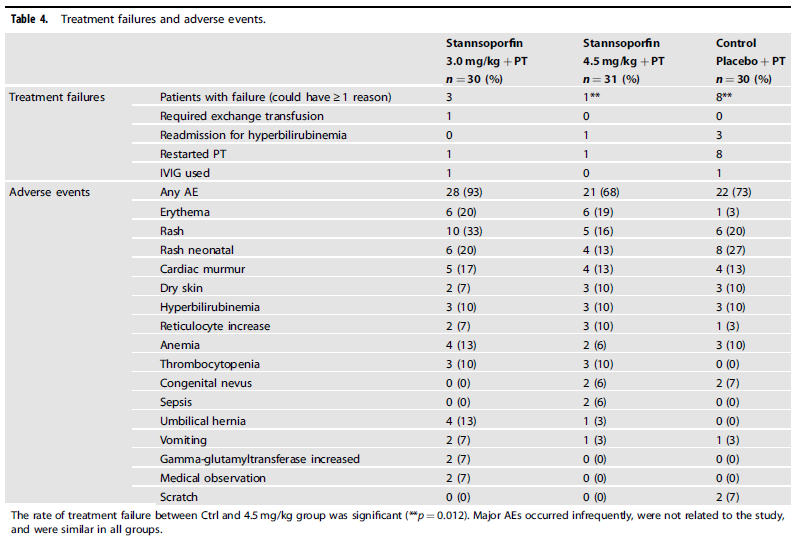
From a side effect standpoint, the following was noted:
Looking at the data, rashes and flushing may be relatively more common yet are transient. Curiously, the number of treatment failures in the control arm was significantly higher meaning of the 30 patients treated with phototherapy alone, 8 had to restart after the predetermined threshold for stopping phototherapy was reached.
Is this ready for prime time?
The purpose of sharing this information with you is not to promote it as a treatment that we should all jump on. I think this story is still early. What will be needed from here are larger studies with well designed follow-up targeting long term outcomes. This study will be following up patients to see how they did but larger numbers will no doubt be wanted before people embrace this wholeheartedly. A quick search of trials on clinicaltrials.gov shows that there are several trials completed and no doubt some to come. Having an exchange transfusion is no laughing matter as there are risks related to clotting, bleeding, platelets etc so having another tool in our toolkit to deal with this common issue in neonates is of interest to me. Maybe it is of interest to you as well.
Phototherapy is one of the “bread and butter” treatments in the newborn. For sure it has gone through changes over the years as different light sources have been developed that provide more limited spectrums of blue/green light wavelengths. Gone are the old long white tubes in favour of special blue light emitting banks of lights and with it bilirubin levels are effectively dropping quickly worldwide. There have been a couple concerns raised with phototherapy over the years. One concern has been the risk of DNA damage as shown by Ramy N et al in Jaundice, phototherapy and DNA damage in full-term neonates. It was found in this study that the duration of phototherapy but not it’s intensity were related to the extent of methylation of DNA which is a marker of damage. Shorter durations would therefore be preferable. Repair of damaged DNA is thought in some ways to contribute to risk of cancer so although this has not been demonstrated with phototherapy the concern has been raised before. The other concern pertains to the ELBW infant with very thin skin. In the randomized trial for babies under 1000g entitled Aggressive vs. conservative phototherapy for infants with extremely low birth weight. In this trial a lower threshold for starting phototherapy was used in the “aggressive group”. The findings of this study in a preplanned subgroup analysis was that the babies from 500-750g that had a lower threshold for starting and continuing phototherapy had a trend towards a higher mortality; relative risk, 1.13; 95% CI, 0.96 to 1.34 as the CI just crossed 1. With this information in the literature it stands to reason that the question would come up as to whether continuous phototherapy is needed or whether one could use cycled intermittent phototherapy to give infants “phototherapy breaks”.
Such a study has now been published
This study Cycled Phototherapy Dose-Finding Study for Extremely Low-Birth-Weight Infants A Randomized Clinical Trial enrolled babies with birthweights between 401 – 1000g and Initially randomized using a 1:1:1 ratio to 3 treatment groups: continuous PT (usual care), a PT regimen of 30 minutes or more per hour for each cycle, or a PT regimen of 15 min/h or more. The minutes per hour of PT could be increased for the cycled if TSB values reached specified thresholds. After the first 100 patients a planned analysis was done and the 30 minute group was ended as there was no difference between this group and the 15 minute one. The light sources and spectral irradiance (combination of intensity and distance from the patient) used were all the same and collection times for serum bilirubin levels were standardized as much as possible. Bilirubin levels were collected daily for the first 7 days and anytime infants were on phototherapy. The authors also included a stepwise prolongation of phototherapy for the shorter cycled groups if bilirubin levels were not responding to the provided phototherapy. I have to say they really did a good job of removing as many potential variables to outcome as they could!
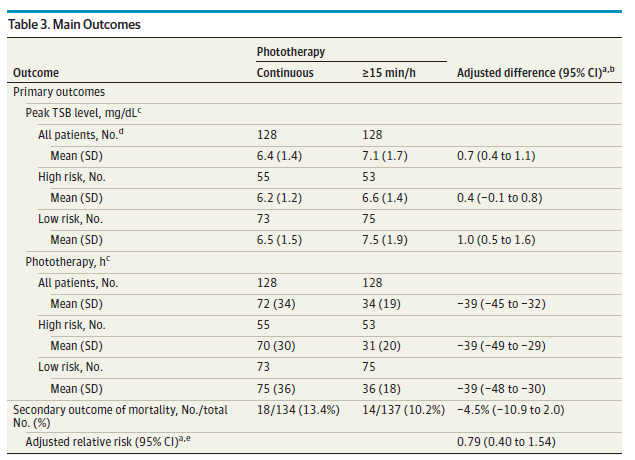
The primary outcomes were mean peak TSB levels and mean PT hours through day 14 across all centers and predischarge wave V latency brainstem auditory evoked potential (BAER). In total 305 infants were randomized in the study and the interestingly the study was stopped at that point as a larger study was approved to obtain more precise estimates in the future around mortality and morbidity as a primary outcome. During the trial the authors received approval to do so with this new primary outcome and so we have what we have to analyze.
The Results
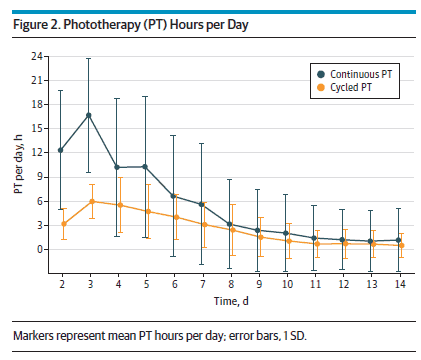
The authors found that there was no difference in the mean peak bilirubin even among high risk patients when given cycled phototherapy for 15 minutes an hour vs continuous. The total amount of hours of phototherapy was approximately halved. No statistical difference in mortality was observed although as mentioned above this was not the primary endpoint of the study.
Looking at duration of phototherapy in terms of hours per day over the first two weeks is shown below. Although a pre-specified plan was in place to increase time as needed to decrease bilirubin levels the amount of time remained fairly consistent for the cycled group with some increase needed in the early days which would be expected given the typical higher biirbubin tendency in the first week of life.
The BAER tests did not demonsrate any difference between the children who had cycled or continuous phototherapy suggesting that no added neurotoxicity occurred from interrupting phototherapy.
What can we take from this?
All of these infants were ELBW and wth that had very thin skin. Would cycled phototherapy be as effective in more mature infants? As the authors of the study point out, there have already been several trials in more mature infants demonstrating such effects and arguing that continuous phototherapy is not needed. At the very least this paper and the others before it would argue that interrupting phototherapy to allow breastfeeding or some skin to skin time with the mother or father should be acceptable. In the past I can remember many instances of having ordered intensive phototherapy and then questioned whether mom can breastfeed as technically it is supposed to be continuous. With this information I would suggest that continuing to work on oral feeding skills at the breast is reasonable. Clearly this won’t work in the population studied here as they are too small but for the larger infants there would not seem to be harm.
I suspect the larger study to come may change practice if a higher mortality is indeed shown for continuous phototherapy but for now we will need to wait and see. In a few years we will get the chance to review that study here.
As the saying goes “What is old is new again” and that may be applicable here when talking about prevention of kernicterus. In the 1990s there was a great interest in a class of drugs called mesoporphyrins in the management of hyperbilirubinemia. The focus of treatment for many years had been elimination of bilirubin through the use of phototherapy but this shifted with the recognition that one could work on the other side of the equation. That is to prevent the production of bilirubin in the first place.
Tin mesoporphyrins (SnMP) have the characteristic of being able to inhibit the enzyme hemo oxygenase quite effectively. By achieving such blockade the breakdown of heme to carbon monoxide and biliverdin (the precursor of bilirubin) is inhibited. In so doing, the production of bilirubin is reduced making one less dependent on phototherapy to rid the body of elevated levels. So simple and as you might imagine a good reason for there to have been significant interest in the product. One article by Martinez et al entitled Control of severe hyperbilirubinemia in full-term newborns with the inhibitor of bilirubin production Sn-mesoporphyrin. was published in 1999 and demonstrated that infants with severe hyperbilirubinemia between 48-96 hours could have their need for phototherapy eliminated by use of the product compared to 27% of the infants in the control group needing treatment. Additionally, total bilirubin samples were reduced from a median of 5 to 3 with the use of one IM injection of SnMP. This small study was hampered though by inability to really look at adverse outcomes despite its effectiveness. What has been seen however is that SnMP if given to infants who are then treated with white lights can create a rash which is not seen however when special blue light is employed.
Two other studies followed exploring the use of SnMP in cases of severe hyperbilirubinemia in term infants and were the subject of a Cochrane review in 2003. The conclusions of the review essentially became the death nell for the therapy as they were as follows.
“…may reduce neonatal bilirubin levels and decrease the need for phototherapy and hospitalization. There is no evidence to support or refute the possibility that treatment with a metalloporphyrin decreases the risk of neonatal kernicterus or of long-term neurodevelopmental impairment due to bilirubin encephalopathy… Routine treatment of neonatal unconjugated hyperbilirubinemia with a metalloporphyrin cannot be recommended at present.”
The literature after this basically dries up, that is until this month when a paper emerges that is best described as a story of mystery and intrigue!
Prophylactic Use of SnMP From 2003 Published in 2016!
This paper as you read it almost seems like a conspiracy story. The paper is by Bhutani et al (as in the nomogram) Clinical trial of tin mesoporphyrin to prevent neonatal hyperbilirubinemia. The study set out to answer a different question than had been previously studied. The question here was, if you provided a single IM dose of SnMP to infants who were at or above the 75%ile on the risk nomogram, could you prevent the need for phototherapy or exchange transfusion as the primary outcome. Secondarily, the authors truly wanted to demonstrate safety of the product and planned on recruiting 800 patients per arm in the study. The study appeared to be well planned and as with many studies had a safety monitoring committee which was to do interim analyses. After the first analysis the FDA became involved and recommended studies to look at a prophylactic versus therapeutic approach. Due to the interim analysis the study had been halted and after the FDA made their suggestion the study was simply never restarted as future studies were planned to look at the effectiveness and safety of the two approaches. The authors state that they planned on reporting their results in 2006/7 but elected to wait until long term data emerged. Now finally 9 years later they decided to release the results of the partially completed study. The story around this study I find as interesting as the results they obtained!
So What Happened?
Before closing the study they managed to recruit 87 into the intervention arm and 89 into the placebo group and lost none to follow-up. One dose of SnMP had a significant effect on the trajectory of curves for bilirubin production as can be seen in the first figure.
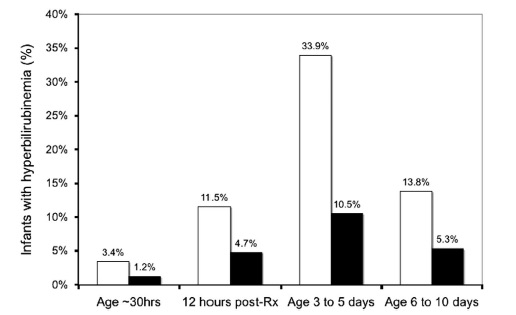
The graph below demonstrates what percentage of patients had a bilirubin level above 220 umol/L (12.9 mg/dl) after the single injection of SnMP (black bars) compared to placebo (white bars).
What can we do with these results?
It would be tough to argue anything other than this being an effective treatment to prevent significant hyperbilirubinemia. Unfortunately, like many studies that were never completed this one remains underpowered to conclusively demonstrate that the use of SnMP is safe in both the short and long term periods. The absence of such data make it very difficult to recommend SnMP as standard of care. One has to add to this that while we have evidence to show it reduces the rate of rise of bilirubin, what we don’t know is whether in a larger study the incidence of bilirubins > 425 umol/L or the need for exchange transfusion might be reduced. If this were the case, it would make for a compelling argument to try SnMP.
That is the approach for standard of care though. In the setting of a patient with a known blood group incompatibility who was at high risk for exchange transfusion, if they received IVIG and the bilirubin continued to climb might there be a role here? I would tend to say yes if we could get our hands on some. The authors by sharing this data have shown the medication is effective in doing what it is supposed to do. Given that at least in our centre all of our lights are of the new variety, the risk of rash would be nonexistent. The risk for kernicterus or at least an exchange transfusion though would not be minimal so if we have this in our toolbox I would after weighing the risks opt to give it.
I certainly wonder if there are places out there who have used it and if so what is your experience?
I have been mulling over this piece for some time. In my own practice I have long questioned the role for standard phototherapy (the equivalent of a single light source) vs intensive phototherapy (delivering >30 microwatts/cm2/nm and usually two light sources) when treating jaundice for all patients. I have bolded that last part to emphasize that I am not just talking about newborns with severe hyperbilirubinemia but rather all infants with treatable jaundice based on local treatment curves such as shown in the CPS and AAP statements.
When newborns are only 30 – 50 micromol/L above the treatment threshold as an example, I will see standard phototherapy ordered or after initiating treatment with intensive phototherapy as the level approaches no treatment required you will see people switch to standard phototherapy again. Why is that and does it make sense?
The rationale for using less intensive phototherapy has been to minimize side effects. Historically, these were retinal damage (hence the eye covers), electrolyte disturbances, increased insensible water loss and occasionally rashes. I use the word historically as they for the most part are no longer relevant today provided a narrow spectrum LED light source is utilized which is the technology used in most modern phototherapy light sources now. Backing up this claim, in 2008 Dr. Maisels, showed that in preterm infants receiving LED based light there were no increases in transepidermal water loss. By limiting the wavelength of light emitted to 430 – 490 nm and avoiding the infrared wavelengths. Whether the concern exists with respect to retinal effects is tough to say for sure so continued precautions with eye covers are recommended.
Go Big or Go Home
If there is little harm to phototherapy then is there a reason to use more? The effectiveness of phototherapy is generally based on three things. The first is the proximity of the light source to the patient (< 15 cm is ideal), the second is the intensity of the lamp and the third is the surface area covered. If you are using a single focused spot and covering only 15- 20% of the body you are missing out on a lot of skin that could be helping to lower an infants bilirubin more rapidly. As I see it, if there is little harm in giving phototherapy and the rate of bilirubin decline is faster with better phototherapy, why would you use anything less than intensive using two light sources? Also from a developmental care point of view, less time under the lights means more time for skin to skin and that is always a good thing.
Phototherapy and DNA damage
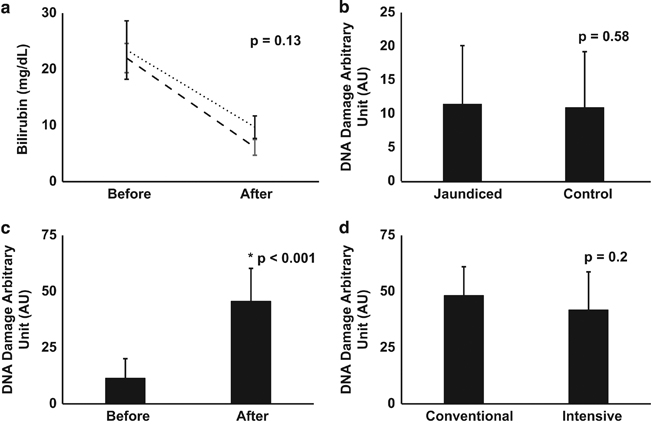
What prompted me to write this piece actually was the following paper Jaundice, phototherapy and DNA damage in full-term neonates by Ramy N et al from November of 2015. In this paper the authors used a validated measure of DNA damage and assessed infants both before and after phototherapy. Thirty six newborns with jaundice were compared to 30 controls. The results are shown in the following figure.
Figure B demonstrates that prior to initiation of phototherapy the extent of DNA damage in tested cells is no different whether you are jaundiced or not. In essence bilirubin is not toxic to cells which also makes sense knowing that bilirubin has antioxidant properties and hence one would think it might be protective against DNA damage. It is figure C and D that provide the most interesting information. Figure C demonstrates that phototherapy (conventional and intensive groups combined) leads to an increase in DNA damage. Figure D is important in that it illustrates that comparing conventional and intensive phototherapy groups there is no difference in rates of DNA damage. This would indicate that more intensive phototherapy is not hazardous to cells.
What was noted in the end though is what is most important here. As expected the duration of phototherapy differed between the two strategies. Infants in the conventional group were under lights for 62.2 ± 23.02 hrs vs 41.3 ± 22.9 hrs, P = 0.005 in the intensive group. When the authors analyzed the relationship between DNA damage and length of phototherapy there was a statistically significant relationship between the two.
In summary then
Intensive phototherapy is more effective than conventional at reducing levels of jaundice
Phototherapy is associated with minimal clinical side effects whether intensive or conventional.
Infants receiving conventional phototherapy require longer courses of treatment.
Longer courses are associated with greater levels of DNA damage.
The significance of this DNA damage is unknown based on this study but in principal avoiding such injury may be a wise thing to do.
One last benefit – less needle pokes and shorter lengths of stay!
If an infant spends an average of one less day under phototherapy lights do not underestimate the added benefit with respect to avoiding needle pokes. Typically such infants receive one poke a day to “check how the decline is going”. Shortening the course of phototherapy may translate into one or two less pokes or more and that is definitely a good thing!
Lastly I will leave you with a tip from my own practice which I have found very useful to eliminate at least one poke. When phototherapy is effective and the bilirubin is coming down (and is close to the threshold for stopping but not quite there yet) it is common for people on rounds to order another bilirubin for the morning and continue phototherapy until that result. The result comes back the following morning and the practitioner orders a follow-up bilirubin for the following day to check for the “rebound”.
An alternative strategy is to keep the infant on phototherapy overnight and rather than checking on the bilirubin in the morning just stop the phototherapy on rounds. Eight hours later check the bilirubin and if it is below the threshold for treatment send the infant home. You avoid an overnight stay and instead of poking twice in two days do it all in one.
Whether you take this advice or not is up to you but if all that comes from this post is a decrease in the general fear of intensive phototherapy I may have gotten somewhere and the DNA of many babies out there will thank you!
Elon Musk, a name synonymous with technology in our time (as the brains behind the all-electric Tesla automobile), had this to say about the “Good Old Days”
“If anyone thinks they’d rather be in a different part of history, they’re probably not a very good student of history. Life sucked in the old days. People knew very little, and you were likely to die at a young age of some horrible disease…”
I wonder what he would say though about Sister J Ward who worked in the premature unit at Rochford General Hospital, Essex in the 1950s. It was during this time that she took a baby outside with her to enjoy a warm afternoon. Upon returning to the unit and taking off the sheet that accompanied the child she noticed a discrepancy between the yellow colour which remained under the covered skin and that which had been exposed to sunlight. Her observation led her to conclude that the sunlight had in fact been responsible for the change (and she was right!) but her conclusion was largely ignored.
Soon thereafter a tube of blood provided the convincing evidence that the sun was in fact directly responsible for such a change. This tube which had been left on the windowsill in the sun was tested for a bilirubin level and found to be low. As the care providers felt the test was inaccurate a repeat sample was drawn and the fresh tube contained a much higher level. A repeat sample of the blood that was again left in the sun showed an even lower level than previously seen inspiring researchers to seek out the effect of light on bilirubin. This ushered in the age of phototherapy lamps that are used around the world today. The design of such lamps has undergone many changes with the current models mostly focusing on the generation of light in the blue spectrum. Mostly gone in the developed world are the long phototherapy bright light tubes that were ubiquitous when I was in residency. It didn’t start off that way though. All you needed was a little golden sun!
A Randomized Trial of Sunlight to….
This month in the New England Journal of Medicine a non-inferiority study has been published comparing conventional phototherapy with BiliBlankets to you guessed it…sunlight. The study took place in Nigeria where such a study is both practical and possible. Conducting the study in Winnipeg for example would yield a treatment that could be used for 3-4 months a year at best but in a more temperate part of the world it indeed is a reasonable question to ask. The infants randomized to sunlight were placed under filtered light using either a canopy made of an Air Blue 80 film on overcast days or when sunny, in a Gila Titanium film. These films have been shown to essentially block all UV light while allowing light in the blue spectrum through. Aside from Sister Ward demonstrating that sunlight was an effective treatment for jaundice over 60 years ago, a significant motivation for determining if sunlight could be employed is the cost difference of the two strategies. A BiliBlanket will cost between 2-3000 dollars each while these canopies can be made for $0.55 and $1.50 per square foot of film type respectively and $44 and $120 for a canopy for six to eight mother–infant pairs with Titanium and Air Blue 80 films. In countries where resources are scarce one can see the compelling reason to try such a strategy.
The Results
The criteria for efficacy were twofold. The first outcome was achieving a rate of increase in total serum bilirubin of less than 0.2 mg per deciliter per hour for infants up to 72 hours of age or secondly a decrease in total serum bilirubin for infants older than 72 hours of age who were receiving at least 5 hours of phototherapy. After comparing 250 courses using sunlight to 311, five hour exposures to BiliBlankets, sunlight was found to be equally effective. Interestingly, the spectral irradiance (measure of the intensity of the light source) however was significantly higher in the group receiving sunlight 40 vs. 17 μW per square centimeter per nanometer, P<0.001. Additionally, the total area covered was greater under the canopy which may help to explain why in a secondary analysis the rate of decline in bilirubin was found to be faster with sunlight.
But is it safe?
Putting babies under the sun for 5 hours would seem to go against everything we have been taught but remember this was filtered light so sunburn was not a concern. Temperatures were monitored for all children and if necessary they were moved into the shade to cool off or in other cases on quite hot days prophylactic cool towels were applied intermittently. In the end though only one baby recorded a short-lived temperature over 39 degrees, no babies became dehydrated and in only one case was a doctor called to see a child.
Final Thoughts
We are blessed to live in a country where we have ready access to phototherapy blankets, overhead lights that are either independent free units or integrated into expensive neonatal beds. This is not always the case in the developing world. I find it simply amazing that a discovery over 50 years ago that led to the development of an entire industry would one day be simplified back to where it all began. We must not forget that while bilirubin encephalopathy leading to kernicterus is rare in the developed world, in places without access to phototherapy it is a real and present danger. We now know that the most naturopathic treatment of all; the sun which is free and readily available is just as effective and possibly more than our high-tech devices.
Elon Musk may be one of the most brilliant inventors of the modern era but with respect to caring for babies with yellowing of the skin, Sister Ward had a leg up on him.





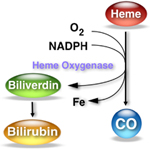 By achieving such blockade the breakdown of heme to carbon monoxide and biliverdin (the precursor of bilirubin) is inhibited. In so doing, the production of bilirubin is reduced making one less dependent on phototherapy to rid the body of elevated levels. So simple and as you might imagine a good reason for there to have been significant interest in the product. One article by Martinez et al entitled
By achieving such blockade the breakdown of heme to carbon monoxide and biliverdin (the precursor of bilirubin) is inhibited. In so doing, the production of bilirubin is reduced making one less dependent on phototherapy to rid the body of elevated levels. So simple and as you might imagine a good reason for there to have been significant interest in the product. One article by Martinez et al entitled 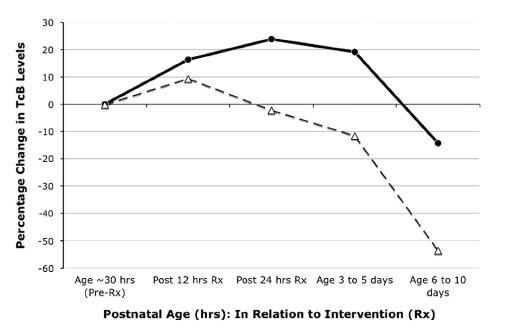

 It was during this time that she took a baby outside with her to enjoy a warm afternoon. Upon returning to the unit and taking off the sheet that accompanied the child she noticed a discrepancy between the yellow colour which remained under the covered skin and that which had been exposed to sunlight. Her observation led her to conclude that the sunlight had in fact been responsible for the change (and she was right!) but her conclusion was largely ignored.
It was during this time that she took a baby outside with her to enjoy a warm afternoon. Upon returning to the unit and taking off the sheet that accompanied the child she noticed a discrepancy between the yellow colour which remained under the covered skin and that which had been exposed to sunlight. Her observation led her to conclude that the sunlight had in fact been responsible for the change (and she was right!) but her conclusion was largely ignored.
