Cool title for a post I think. If you have children or even if you are an adult who likes to play video games you would be aware of virtual reality headsets. These headsets take games to a new level by immersing you in the experience so all you see is the game in your field of vision. It is easy to get lost in this world and lose your sense of the outside world. It seems reasonable then that someone might think to adapt some of the principals of this type of gaming to use in medicine.
I am no stranger to posts on video laryngoscopy having written about it several times already. A search of this site should easily find posts on the topic if you are so inclined. In these posts I think I have made a compelling argument for the use of videolaryngoscopy over direct laryngoscopy to improve inubation success.
A New Way of Doing Things
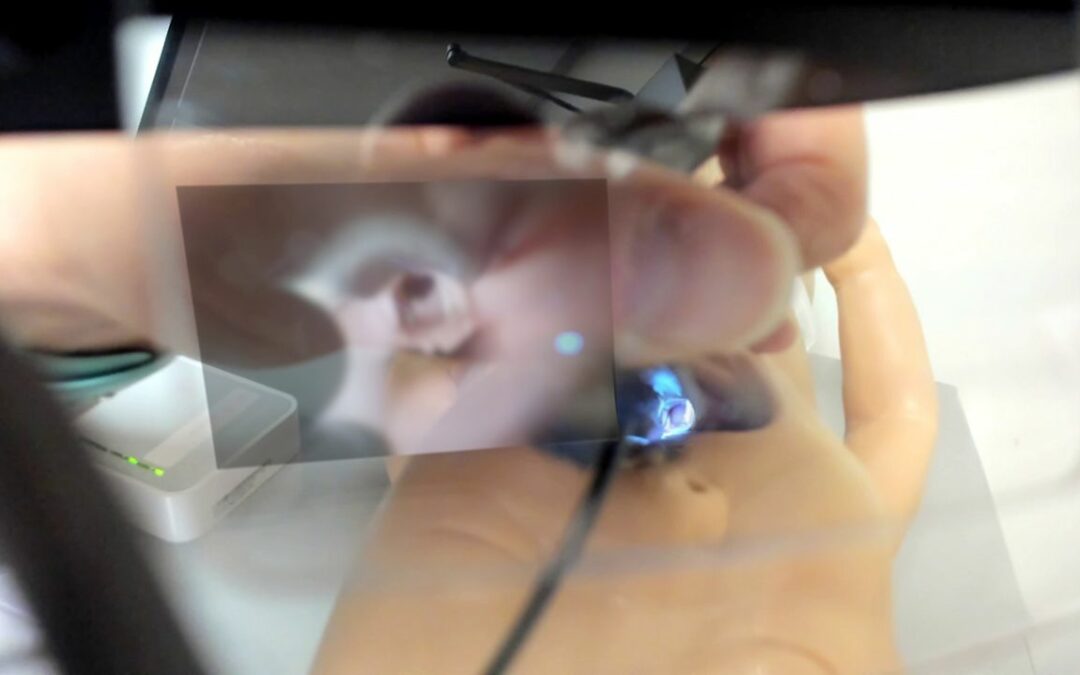
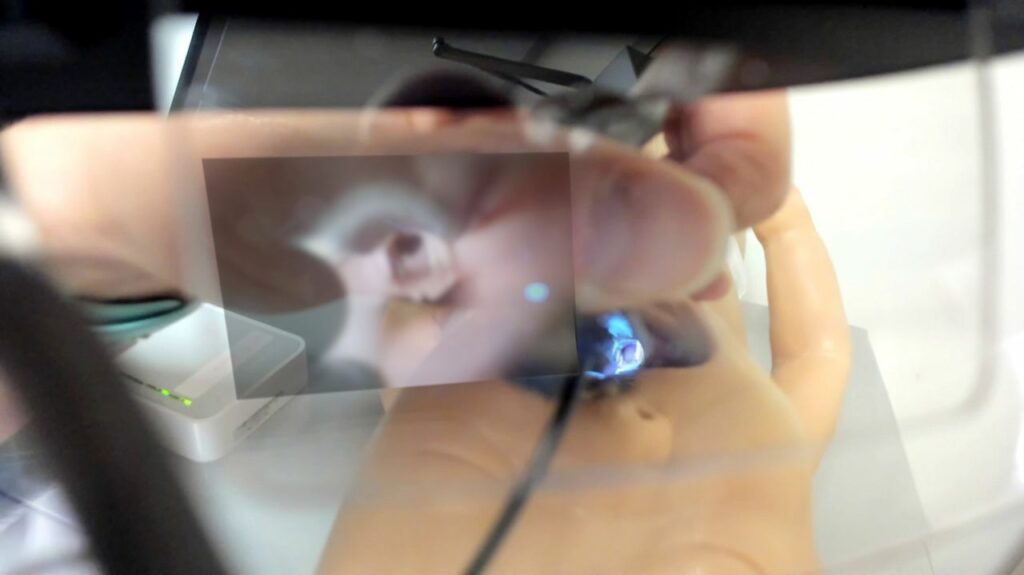
In each of those posts there has been a comparison of two groups in with one uses IVL in which the video image is generally off to the side of where the intubation is taking place and DL or direct layngoscopy with video aid. A new study entitled Augmented Reality–Assisted Video Laryngoscopy and Simulated Neonatal Intubations: A Pilot Study by Patricia L. Dias, et al compares a third method to the other two. The third method is to use a disposbale laryngoscope as shown below with a video camera attached that connects to a tablet. The video captured on the laptop is then sent to glasses the person intubating is wearing that is projected into the line of site as per the image below. In essence its like a car with heads up display. No need to take your eyes off the airway as you are seeing it directly in front of you. Where the tech becomes even more interesting is that the person on the tablet can make notations on the video that appear in the view of the person wearing the glasses. For example one could put an arrow showing where to put the ETT or label the esophagus as such.
In the study there were 45 nursing participants who were assigned to one of three different intubation strategies being DL, IVL and Augmented Reality VL (ARVL). As such there 15 participants in each arm. Each participant was read a script on how to intubate and then had 5 consecutive intubation attempts on a maniken using a miller 1 blade.
How Did They Do
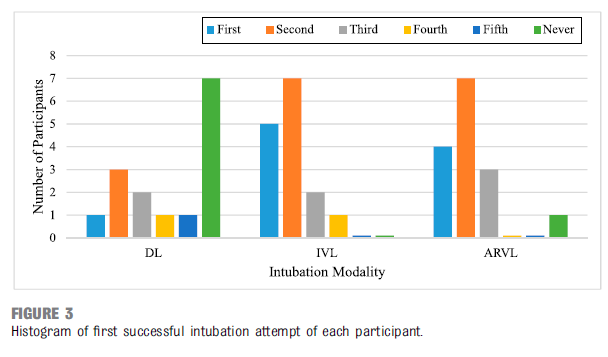
Interestingly there was no difference in success with the ARVL vs the IVL in terms of success on being able to get the ETT into the manequin successfully as shown below but both were better than the DL.
Looking at the details of the success and failure there was also no difference in the two types of videolaryngoscopy.
So Where Does That Leave Us
At the very least what we have seen is once again the ability to intubate is enhanced with VL. There was no difference seen in this group of nurses learning to intubate whether they used a indirect or augmented reality VL. This however is a small study and really to me is a proof of concept study. The authors created a novel method of doing VL although one could argue it is not that differrent that use of the CMAC with the small screen attached to the top of the laryngoscope
The difference though is in the ability of the instructor to write feedback on the tablet and have that show up in the line of sight of the intubator. I see this novel ability as a wonderful educational tool. There is not a learner out there who hasn’t had the experience of looking down at an airway and thinking “what am I looking at?” Sometimes with secretions it can be awfully hard to determine which structure is what. Having someone on a tablet seeing the image you are seeing and rather than having to describe to you what you seeing, they could draw it for you I think is a huge advance. Like many pilots I would suggest this is not the last we have heard of this technology. With this in the literature now I suspect there will be trials to come with more developed devices rather than those put together piecemeal. If these larger trials with less and more advanced intubators demonstrate increased rates of success I could see this becoming the new standard for video laryngoscopy.
The Canadian Pediatric Society has a statement on the use of premedication before non-emergent intubation which was written in 2011 and reaffirmed in 2018. After reviewing available medications for use the recommended strategy was atropine, fentanyl and succinylcholine. This combination does involve three different medications, the first being to prevent bradycardia, the second to sedate and the third to paralyze. With the use of three medications however there is always room for error so it is very alluring to try and use one medication to provide optimal conditions for intubation. As a matter of fact I once tried thiopental as a single agent as a fellow (unpublished) which never saw the light of day due to difficulties with recruitment. Nonetheless I was after a simpler solution to providing good conditions for intubation so it is not surprising that others are also looking at single agents as well.
Propofol Would Seem Like a Good Contender
Propofol has been used in the adult and Pediatric world for some time. It causes a decreased level of conciousness and amnesia surrounding the events for which it was given. It is short acting often wearing off within minutes which would seem perfect for procedural sedation. On the downside one of its side effects is hypotension so in a fragile neonate this might be something to be watch for.
Dose finding study
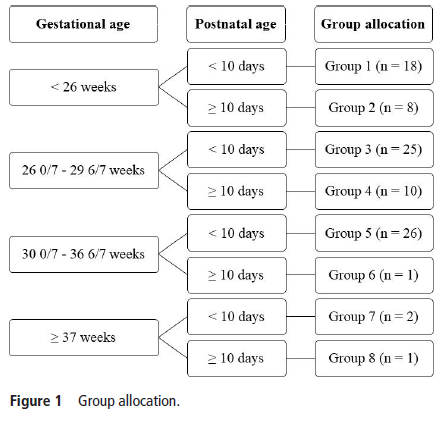
de Kort et al published Propofol for endotracheal intubation in neonates: a dose-finding trial this month. It is an interesting study design for those unfamiliar with dose finding studies. The goal was to begin with a low but starting dose for propofol at 1 mg/kg/dose and escalate by 0.5 mg/kg/dose until adequate sedation was reached WITHOUT signficant adverse side effects. Moreover the authors built on previous work in this area to attempt to break the patients into 8 groups as shown in this figure.
All patients were less than 28 days so allocation was based on gestational age and whether a patient was greater or less than 10 days of age at dosing. Level of intubation readiness was evaluated using a standardized tool called the Intubation Readiness Score.
Side effects were hypotension, myoclonus, chest wall rigidity, persistent respiratory and/or circulatory failure and bronchospasm. Blood pressure was assessed via an indwelling catheter if available or by cuff if not available. Importantly any mean blood pressure after provision of propofol less than the gestational age met the criteria for declaring hypotension.
The Findings
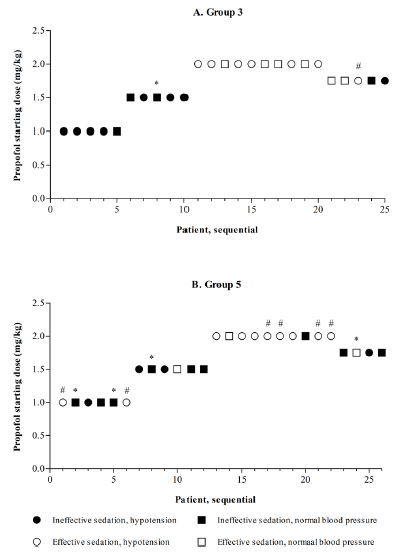
The study was terminated early due to low inclusion in some groups after 91 total patients had been enrolled. In the end there were only enough patients in Groups 3 (26 – 29 weeks and <10 days) and 5 (30 – 36 weeks and < 10 days) enrolled to analyze fully. The results of the dose finding analysis are shown below.
Walking through group 3, there were 5 patients enrolled at the 1 mg/kg level and based on poor levels of sedation in all the dosing for next 5 were increased to 1.5 mg/kg. As intubating conditions improved, the authors found that at a dose of 2 mg/kg while conditions were optimal, hypotension became a significant problem with 59% being hypotensive. The management of hypotension included 54% needing volume resuscitation and inotropes in 10%. Curiously the hypotension often did not appear until 2 hours or more after drug delivery. When the authors did a step down to 1.75 mg/kg as a intubation dose they found it was inadequate for providing good conditions for intubation albeit with less hypotension.
Not the right drug
The goal of this study was to find the optimal dose that provided good intubation conditions without significant side effects. The strength of this study was that it included babies across a wide range of gestational ages from 26+0 to 36+6 weeks gestational age. While the authors were unable to recruit enough patients to fill each group the stoppage of the study made sense as it was clear that the goal of the study would not be met. Propofol would be a great single agent if it weren’t for the issues found in this study. This is not to say that the drug is a poor choice for Pediatrics but in the Neonatal world I just don’t think it has a place. I would welcome further testing on other single agent drugs but that of course is an analysis for another post!
I knew it was a matter of time before a study looking at this strategy came out. Whether you intubate using INSURE or a LISA/MIST technique (passing a semi-rigid catheter through the vocal cords to give surfactant while a baby is on CPAP) there would have to be those that argue the placement of the laryngoscope blade in the mouth and passage of the catheter through the trachea must be uncomfortable. Given such concerns, why wouldn’t you want to provide some sedation to the patient? The main concern would be suppression of respiratory drive and need for intubation or PPV. LISA/MIST usage has been found in systematic reviews to lead to less risk of BPD but what if sedation leads to more PPV especially with uncontrolled tidal volumes on these fragile lungs? Will the benefits remain?
Propofol Before MIST
Dekker et al published Sedation during minimal invasive surfactant therapy: a randomised controlled trial in which they looked at infants receiving surfactant administration by MIST in infants born at 26 – 36 weeks with stratification of results into two groups (26–31+6 and 32–36+6 weeks). The intervention was to give a relatively small dose of propofol 1 mg/kg compared to the typical dose of 2.5 mg/kg prior to using MIST. Physicians were unblinded to the intervention but nurses were asked (they were blinded) to determine the COMFORTneo score as a measure of discomfort or pain. The primary outcome was the percentage of infants with a score <14 during the procedure. A power calculation to determine numbers needed for the study indicated 39 per arm and was based on a previous study (not using propofol though). While it does not appear that a sham was used for a placebo arm, sucrose was utilized for additional comfort in both arms.
The Results Please
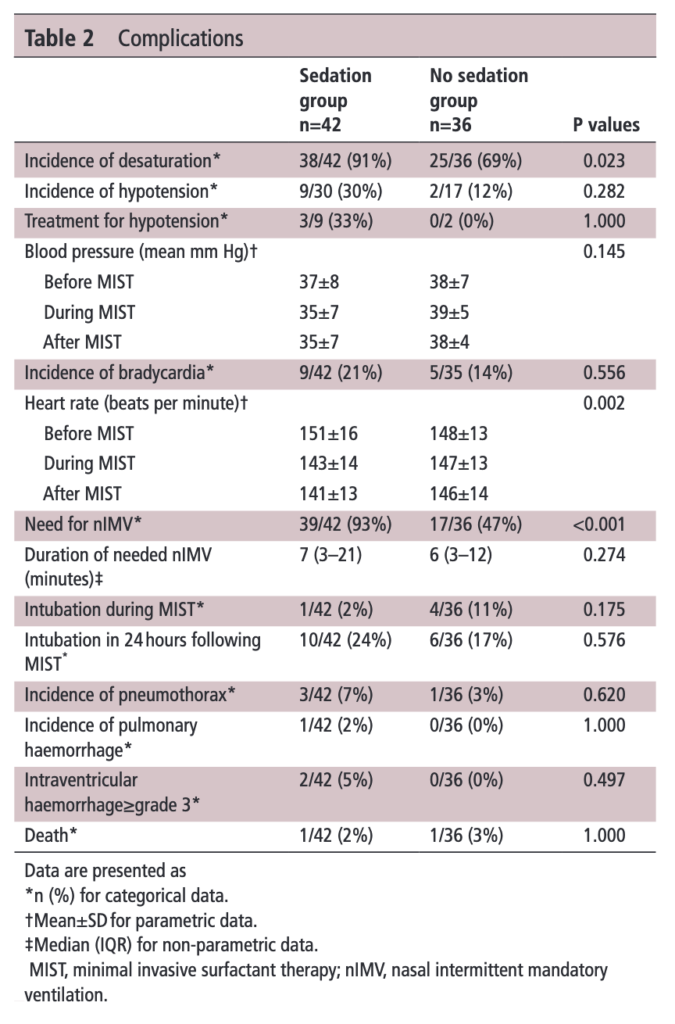
Sedation seemed to work even at this lower dose of propofol as the group who received it had a higher percentage with a score <14 (32/42 (76%) vs 8/36 (22%), p<0.001). Moreover, the overall mean scores were also lower (12±3 vs 17±4; p<0.001). When looking at rates of complications though some interesting but perhaps not surprising findings emerge. A greater risk of desaturation events existed in the group receiving even a low dose of propofol.
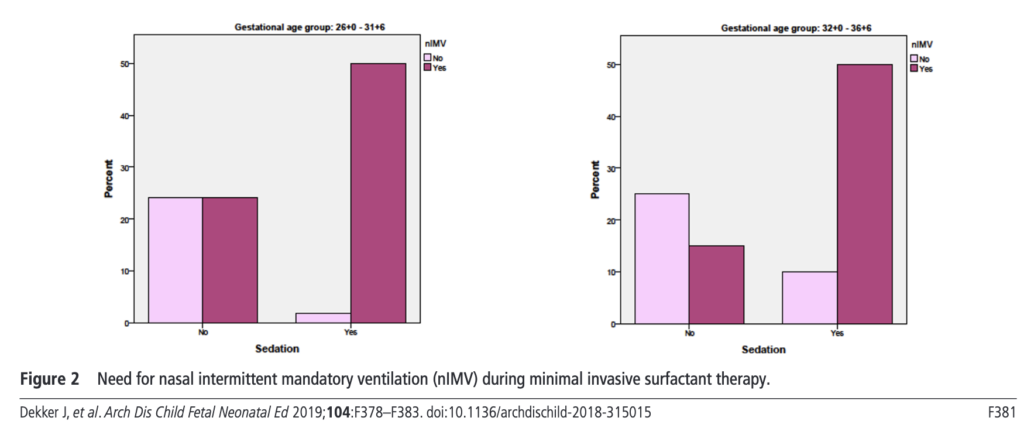
Digesting this information it would seem that giving propofol prior to MIST may defeat the purpose of avoiding positive pressure ventilation as nearly all patients given propofol required nasal intermittent mandatory ventilation. As this is a small study we have to take the secondary outcomes with a grain of salt as the study would not have been powered to detect all these important outcomes such as IVH and pulmonary hemmorhage. Moreover the real question here would be whether BPD would be different between the groups but again not reported and even if it had been the numbers would be a little low to see a real difference.
The next steps I think will be to look at this question using medications such as atropine and fentanyl which I understand in other centres are in use. To do so though will require some pretty big numbers for enrolment. in the meantime what are we to do? Putting a catheter into the trachea I would think would be uncomfortable if not painful. Something should be given prior to the procedure but it is now on the research community to determine what that is and a what dose!
A real change is coming and with this post you will get a glimpse into where the next big thing in Neonatology is likely to be. A catchy title for sure and also an exaggeration as I don’t see us abandoning the endotracheal tube just yet. There has been a lot of talk about less invasive means of giving surfactant and the last few years have seen several papers relating to giving surfactant via a catheter placed in the trachea (MIST or LISA techniques as examples). There may be a new kid on the block so to speak and that is aerosolized surfactant. This has been talked about for some time as well but the challenge had been figuring out how to aerosolize the fluid in such a way that a significant amount of the surfactant would actually enter the trachea. This was really a dream of many Neonatologists and based on a recently published paper the time may be now for this technique to take off.
A Randomized Trial of Aerosolized Surfacant
Minocchieri et al as part of the CureNeb study team published Nebulised surfactant to reduce severity of respiratory distress: a blinded, parallel, randomised controlled trial. This trial set out to obtain a sample size of 70 patients between 29 0/7 to 33 6/7 weeks to demonstrate a difference in need for intubation from 30% down to 5% in patients treated with CPAP (30% was based on the historical average). The authors recognizing that the babies in this GA bracket might behave differently, further stratified the randomization into two groups being 29 0/7 – 31 6/7 weeks and 32 0/7 to 33 6/7 weeks. Those babies who were on CPAP and met the following criteria for intubation were either intubated in the control group and given surfactant (curosurf) using the same protocol as those nebulized or had surfactant delivered via nebulisation (200 mg/kg: poractant alfa) using a customised vibrating membrane nebuliser (eFlow neonatal). Surfactant nebulisation(100 mg/kg) was repeated after 12 hours if oxygen was still required. The primary dichotomous outcome was the need for intubation within 72 hours of life, and the primary continuous outcome was the mean duration of mechanical ventilation at 72 hours of age.
Criteria for intubation
1. FiO2 >0.35 over more than 30 min OR FiO2 >0.45 at
anytime.
2. More than four apnea/hour OR two apnea requiring BVM
3. Two cap gases with pH <7.2 and PaCO2 >65 mm Hg (or) >60 mm Hg if arterial blood gas sample).
4. Intubation deemed necessary by the attending physician.
Did It Work?
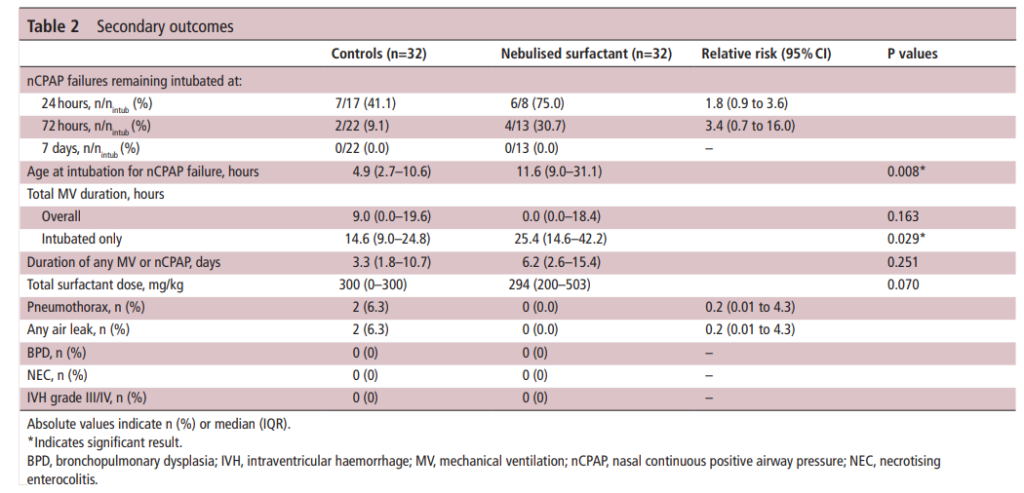
Eureka! It seemed to work as 11 of 32 infants were intubated in the surfactant nebulisation group within 72 hours of birth vs.22 out of 32 infants receiving CPAP alone (RR (95% CI)=0.526 (0.292 to 0.950)). The reduction though was accounted for by the bigger babies in the 32 0/7 to 33 6/7 weeks group as only 1 of 11 was intubated when given nebulized surfactant compared to 10 of 13 managed with CPAP. The duration of ventilation in the first 72 hours was not different between the groups: the median (range) 0 (0–62) hour for the nebulization group and 9 (0–64) hours for the control group (p=0.220). It is important in seeing these results that the clinicians deciding whether infants should be intubated for surfactant administration were blind to the arm the infants were in. All administration of curosurf via nebulization or sham procedures were done behind a screen.
The total number of infants randomized were 66 so they did fall shy of the necessary recruitment but since they did find a difference the results seem valid. Importantly, there were no differences in complications although I can’t be totally confident there really is no risk as this study was grossly underpowered to look at rarer outcomes.
Breaking down the results
This study has me excited as what it shows is that “it kind of works“. Why would larger babies be the ones to benefit the most? My guess is that some but not a lot of surfactant administered via nebulization reaches the alveoli. Infants with lesser degrees of surfactant deficiency (32 0/7 to 33 6/7) weeks might get just enough to manage without an endotracheal tube. Those infants (in particular less than 32 0/7 weeks) who have more significant surfactant deficiency don’t get enough and therefore are intubated. Supporting this notion is the overall delay in time to intubation in those who were intubated despite nebulization (11.6 hours in the nebulization group vs 4.9 hours in the control arm). They likely received some deposition in the distal alveoli but not enough to completely stave off an endotracheal tube.
One concerning point from the study though had to do with the group of infants who were intubated despite nebulization of surfactant. When you look at total duration of ventilation (hours) it was 14.6 (9.0–24.8) in the control arm vs 25.4 (14.6–42.2) p= 0.029*. In other words infants who were intubated in the end spent about twice as long intubated as those who were intubated straight away. Not a huge concern if you are born at 32 weeks or more but those additional thousands of positive pressure breaths are more worrisome as a risk for CLD down the road.
As it stands, if you had an infant who was 33 weeks and grunting with an FiO2 of 35% might you try this if you could get your hands on the nebulizer? It appears to work so the only question is whether you are confident enough that the risk of such things as pneumothorax or IVH isn’t higher if intubation is delayed. It will be interesting to see if this gets adopted at this point.
The future no doubt will see a refinement of the nebulizer and an attempt to see how well this technique works in infants below 29 weeks. It is in this group though that prolonging time intubated would be more worrisome. I don’t want to dismiss this outright as I see this as a pilot study that will lead the way for future work that will refine this technique. If we get this right this would be really transformative to Neonatology and just might be the next big leap.
The modern NICU is one that is full of patients on CPAP these days. As I have mentioned before, the opportunity to intubate is therefore becoming more and more rare is non-invasive pressure support becomes the mainstay of therapy. Even for those with established skills in placing an endotracheal tube, the number of times one gets to do this per year is certainly becoming fewer and fewer. Coming to the rescue is the promise of easier intubations by being able to visualize an airway on a screen using a video laryngoscope. The advantage to the user is that anyone who is watching can give you some great tips and armed with this knowledge you may be better able to determine how to adjust your approach.
For those of you who have followed the blog for some time, you will recall this is not the first time video laryngoscopy has come up. I have spoken about this before in Can Video Laryngoscopy Improve Trainee Success in Intubation. In that piece, the case was made that training residents how to intubate using a video laryngoscope (VL) improves their success rate. An additional question that one might ask though has to do with the quality of the intubation. What if you can place a tube using a video laryngoscope but the patient suffers in some way from having that piece of equipment in the mouth? Lucky for us some researchers from the Children’s Hospital of Philadelphia have completed a study that can help answer this additional question.
Video Laryngoscopy may work but does it cause more harm than good?
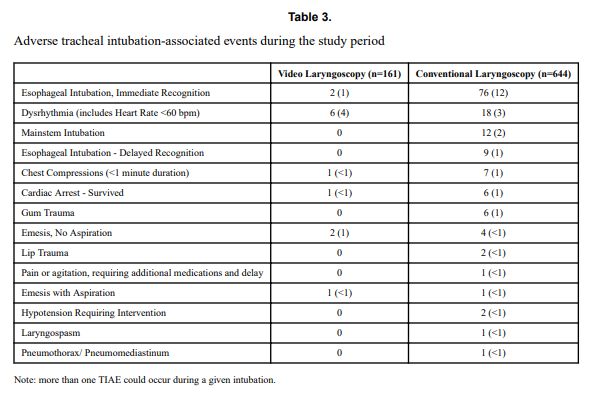
Using a video laryngoscope requires purchasing one first and they aren’t necessarily cheap. If they were to provide a better patient experience though the added cost might well be worth it. Pouppirt NR et al published Association Between Video Laryngoscopy and Adverse Tracheal Intubation-Associated Events in the Neonatal Care Unit. This study was a retrospective comparison of two groups; one having an intubation performed with a VL (n=161 or 20% of the group) and the other with a standard laryngoscope (644 or 80% of the group). The study relied on the use of the National Emergency Airway Registry for Neonates (NEAR4NEOs), which records all intubations from a number of centres using an online database and allows for analysis of many different aspects of intubations in neonates. In this case the data utilized though was from their centre only to minimize variation in premedication and practitioner experience.
Tracheal intubation adverse events (TIAEs) were subdivided into severe (cardiac arrest, esophageal intubation with delayed recognition, emesis with witnessed aspiration, hypotension requiring intervention (fluid and/or vasopressors), laryngospasm, malignant hyperthermia, pneumothorax/pneumomediastinum, or direct airway injury) vs non-severe (mainstem bronchial intubation, esophageal intubation with immediate recognition, emesis without aspiration, hypertension requiring therapy, epistaxis, lip trauma, gum or oral trauma, dysrhythmia, and pain and/or agitation requiring additional medication and causing a delay in intubation.
Looking at the patient characteristics and outcomes, some interesting findings emerge.
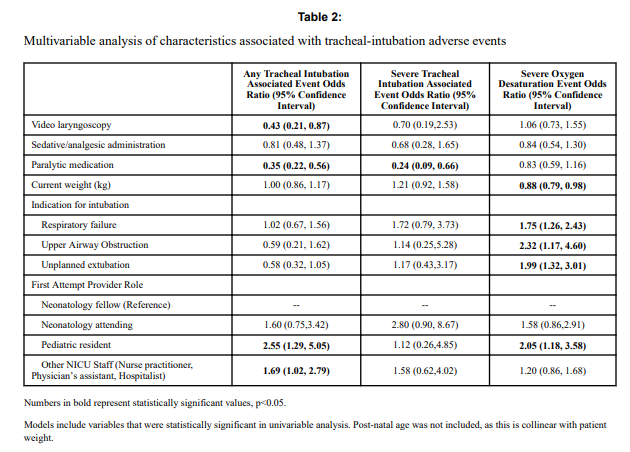
Patients who had the use of the VL were older and weighed more. They were more likely to have the VL used for airway obstruction than respiratory failure and importantly were also more likely to receive sedation/analgesia and paralysis. These researchers have also recently shown that the use of paralysis is associated with less TIAEs so one needs to bear this in mind when looking at the rates of TIAEs. There were a statistically significant difference in TIAEs of any type of 6% in the VL group to 19% in the traditional laryngoscopy arm but severe TIAEs showed not difference.
Given that several of the baseline characteristics might play a role in explaining why VL seemed superior in terms of minimizing risk of TIAEs by two thirds, the authors performed a multivariable analysis in which they took all factors that were different into account and then looked to see if there was still an effect of the VL despite these seemingly important differences. Interestingly, use of VL showed an Odds ratio of 0.43 (0.21,0.87 95% CI) in spite of these differences.
What does it mean?
Video laryngoscopy appears to make a difference to reducing the risk on TIAEs as an independent factor. The most common TIAE was esophageal intubation at 10% and reducing that is a good thing as it leads to fewer intubation attempts. This was also sen as the first attempt success was 63% in the VL group vs 44% in the other.
Now we need to acknowledge that this was not a randomized controlled trial so it could indeed be that there are other factors that the authors have not identified that led to improvements in TIAEs as well. What makes this study so robust though is the rigour with which the centre documents all of their intubations using such a detailed registry. By using one centre much of the variability in practice between units is eliminated so perhaps these results can be trusted. Would your centre achieve these same results? Maybe not but it would certainly be interesting to test drive one of these for a period of time see how it performs.
A few weeks back I wrote about the topic of intubations and whether premedication is really needed (Still performing awake intubations in newborns? Maybe this will change your mind.) I was clear in my belief that it is and offered reasons why. There is another group of practitioners though that generally agree that premedication is beneficial but have a different question. Many believe that analgesia or sedation is needed but question the need for paralysis. The usual argument is that if the intubation doesn’t go well and the patient can’t spontaneously ventilate could we be worse off if the patient loses their muscle tone.
Neonatal Intubation Registry
At the CPS meeting last month in Quebec City. I had the pleasure of listening to a talk by Dr. Elizabeth Foglia on the findings from a Neonatal intubation registry that many centres have been contributing to. The National Emergency Airway Registry for Neonates (NEAR4NEOs), records all intubations from a number of centres using an online database and allows for analysis of many different aspects of intubations in neonates.
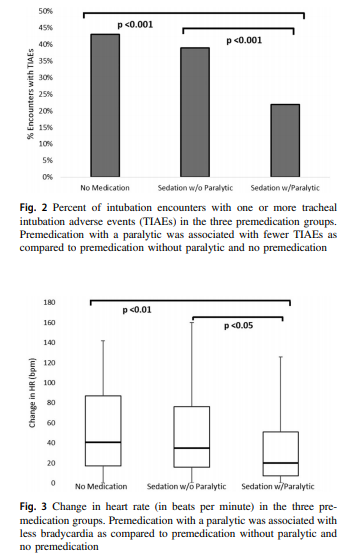
This year, J. Krick et al published Premedication with paralysis improves intubation success and decreases adverse events in very low birth weight infants: a prospective cohort study. This study compared results from the registry of two centres, the University of Washington Medical Center (UWMC) and Seattle Children’s Hospital where the former rarely uses paralysis and the latter in almost all instances of non-emergent intubation. In all, 237 encounters were analyzed in the NICU for babies < 1500g with the majority of encounters (181) being from UWMC. The median PMA at intubation was 28 completed weeks (IQR: 27, 30), chronological age was 9 days (IQR: 2, 26) and weight was 953 g (IQR: 742,1200). The babies were compared based on the following groups. Premedication with a paralytic 21%, without a paralytic 46% and no premedication 31%.
This was an observational study that examined the rates of adverse events and subdivided into severe (cardiac arrest, esophageal intubation with delayed recognition, emesis with witnessed aspiration, hypotension requiring intervention (fluid and/or vasopressors), laryngospasm, malignant hyperthermia, pneumothorax/pneumomediastinum, or direct airway injury) vs non-severe (mainstem bronchial intuba- tion, esophageal intubation with immediate recognition, emesis without aspiration, hypertension requiring therapy, epistaxis, lip trauma, gum or oral trauma, dysrhythmia, and pain and/or agitation requiring additional medication and causing a delay in intubation.).
How did the groups compare?
It turns out paralysis seems to be a big deal (at least in this group of infants). Use of paralysis resulted in less attempts to intubate (median 1 attempt; IQR: 1, 2.25 vs. 2; IQR: 1, 3, p < 0.05)). In fact success was no different between the groups with no paralysis or no premedication at all! When it comes to tracheal intubation adverse events the impact of using paralysis becomes more evident. Paralysis does make a difference in reducing the incidence of such events and moreover when only looking at the rate of severe adverse events as defined above the finding was that none occurred when paralysis was used vs 9 when no paralysis was employed and 5 when no premedication was used at all. The rate of bradycardic events was less in the paralytic group but rates of oxygen desaturation between the three arms were no different.
How do we interpret the results?
Based on the results from the registry it looks like paralysis is a good thing here when electively intubating infants. If we try to determine the reason for it I suspect it may have much to do with the higher likelihood of success on the first attempt at placing an ETT. The longer it takes to place the ETT or the more number of attempts requiring intermittent PPV in a patient who truly needs a tube the greater the likelihood that you will see adverse events including bradycardia. It may simply be that a calm and still patient is an easier intubation and getting the tube in faster yields a more stable patient.
I am biased though and I think it is worth pointing out another possible reason for the differing results. One hospital in this study routinely used premedication and the other did not. Almost 3/4 of the patients came from one hospital which raises the possibility that skill set could be playing a role. If the skill of providers at the two hospitals differed, the results could reflect the variable skill in the practitioners versus the difference in the medications used themselves. What I don’t know though is whether the two share the same training program or not. Are the trainees the same at both sites (google maps says the two sites are 11 minutes away by car)? The difference still might be in local respiratory therapists or Neonatologists intubating as well. Regardless, the study provides evidence that paralysis makes a difference. To convince those out there though who remain skeptical I think we are going to need the registry to take part in a prospective trial using many centres. A format in which several centres that don’t use paralysis are compared to several who do routinely would help to sort out the concern in skill when looking only at two centres. This wouldn’t be randomized of course but I think it would be very difficult at this point to get a centre that strongly believes in using paralysis to randomize so a prospective study using groups chosen by the individual centre might be the next best thing. If anyone using the registry is reading this let me know what you think?










 Paralysis does make a difference in reducing the incidence of such events and moreover when only looking at the rate of severe adverse events as defined above the finding was that none occurred when paralysis was used vs 9 when no paralysis was employed and 5 when no premedication was used at all. The rate of bradycardic events was less in the paralytic group but rates of oxygen desaturation between the three arms were no different.
Paralysis does make a difference in reducing the incidence of such events and moreover when only looking at the rate of severe adverse events as defined above the finding was that none occurred when paralysis was used vs 9 when no paralysis was employed and 5 when no premedication was used at all. The rate of bradycardic events was less in the paralytic group but rates of oxygen desaturation between the three arms were no different.