

I presented this topic as a fellow many years ago after a paper came on the scene suggesting better outcomes with a faster approach. The paper Randomized trial of “slow” versus “fast” feed advancements on the incidence of necrotizing enterocolitis in very low birth weight infants. was plagued by the same issue as others created around those years which was a small number of patients at the lowest gestational ages. Any differences in sub analyses were difficult to really believe as the outcomes could have easily been explained by chance. Having said that, many centres began advancing feeds a little faster than the typical 20 ml/kg/d in favour of 30 ml/kg/d. It would take some time to coordinate a trial large enough to really answer questions about relevant issues such as time to developmental outcomes, time to full feedings and rates of NEC and the time appears to be now.
The SIFT trial
This trial (Controlled Trial of Two Incremental Milk-Feeding Rates in Preterm Infants) was the result of a great deal of coordination between 55 different centres. For inclusion, infants had to be <1500g and <32 weeks gestational age at birth. Once the decision was made to advance feeds, babies were randomized to receive increases of 18 mL/kg/d vs 30 ml/kg/d. The primary outcome was survival without mod-erate or severe neurodevelopmental disability at 24 months CGA. What is striking about the study is its size. The number of babies in the fast arm was 1394 while 1399 in the slower group. In terms of having sufficient numbers of infants who were at the earliest gestational ages they were able to accomplish this as shown in this table.
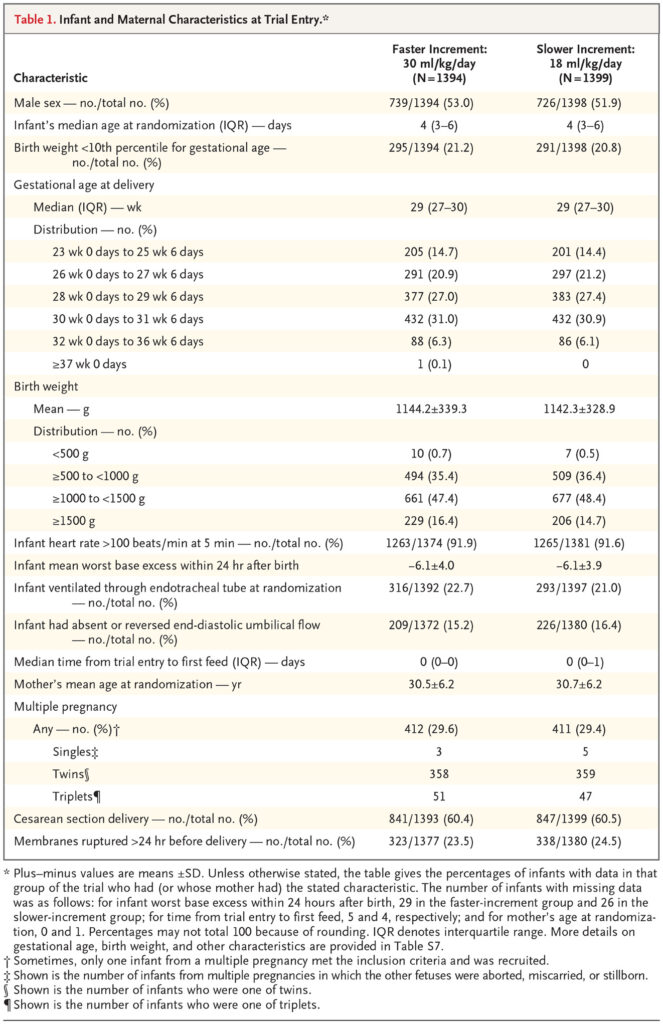
Importantly when looking at the primary outcome 87.4% of infants in the faster group vs 88.7% in the slower group were followed up for assessment. It is also worth mentioning that this is even more impressive in terms of retention when one considers that about 6% in both arms died before assessment.
What were the findings then?
There was no difference in the primary outcome or for that matter each of its’ competing parts.
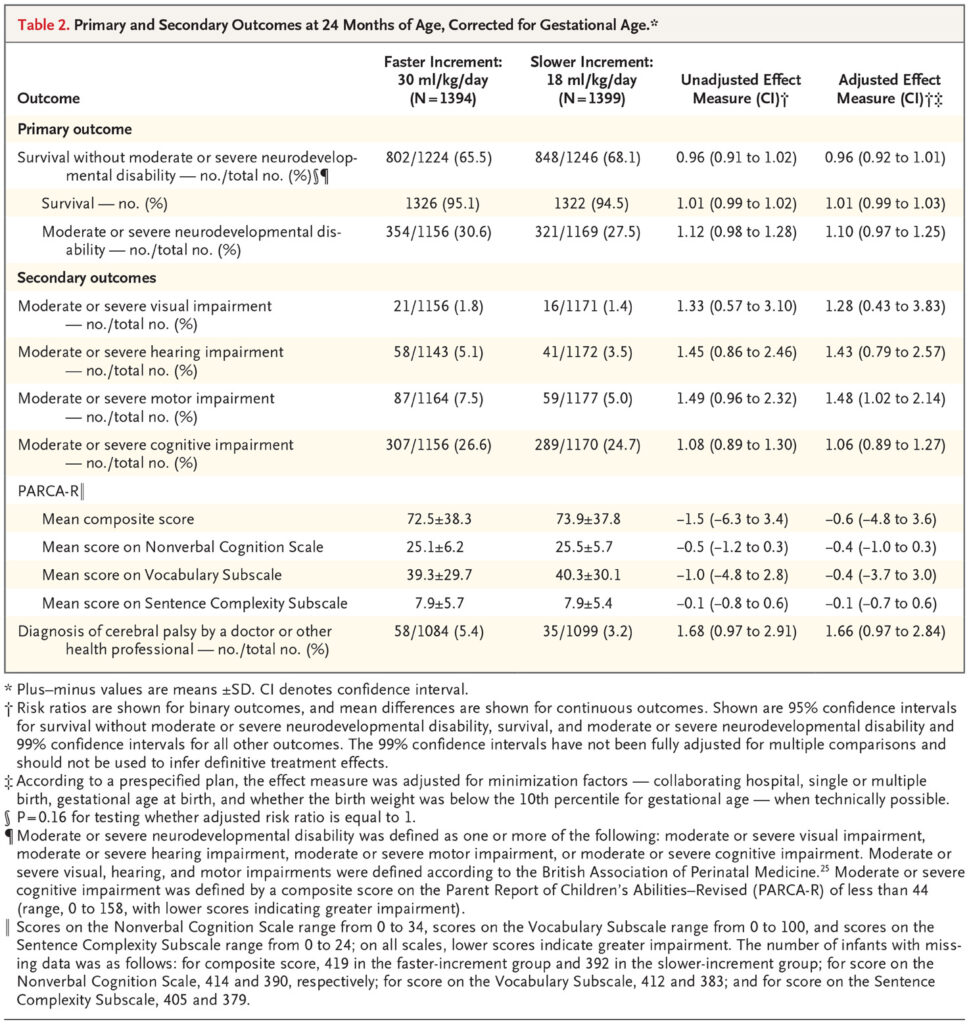
The authors in a secondary analysis did show a very marginal significant finding favouring slow feeds with respect to motor outcome. I concur with the authors though that given the small effect size and the “fishing” for results this likely is simply a chance finding. I can’t think of any reason why that would be the case either from a biological standpoint.
Not surprisingly another significant finding was shorter durations to reach full feeds (10 vs 7 days) and days on TPN at 11 vs 9 in the slow vs fast groups. In spite of having less need for central venous access, the authors were unable to show a reductoin in late onset sepsis or NEC.
Does it change your management?
I suppose that depends on what your management currently is. If you are like our centre and already advancing feedings by 30 ml/kg/d then I suspect not much. If you are in a slow centre one can take away from this study that at the very least you can lessen your patient’s need for central venous access and TPN. Based on this study and my suspicion that there will be no bigger trial forthcoming, whatever you decide to do this is about the best data that you will be getting.