by All Things Neonatal | Nov 23, 2017 | hypoglycemia
We sure do poke a lot of babies to test their blood glucose levels. Some of these babies don’t have so much blood to spare either so checking sugars multiple times a day can drain the body of that precious blood they so need for other functions. Taking too much can always be addressed with a blood transfusion but that as I see it may be avoidable so shouldn’t we do what we can to cut down on blood work? Those with diabetes will be familiar with a continuous glucose monitor (CGM) which is implanted in the skin and can stay in place up to 7 days. The device does require calibration twice a day with a capillary sample to verify it is reading well but this saves a couple pokes a day for those who check four times a day. Such a device could be useful in the NICU where those with hypoglycemia may be checked 6 or more times per day if they are either hypo or hyperglycemic. Cutting this down to two a day would certainly we something worth striving for and if not for the reduction in blood loss then for the minimization of painful procedures.
Does it work in small babies?
A natural question for sure.Uettweller et al published Real-time continuous glucose monitoring reduces the duration of hypoglycemia episodes: a randomized trial in very low birth weight neonates. In babies with a BW < 1500g they were able to demonstrate in 43 babies (21 with traditional intermittent glucose checks vs 22 with CGM) a reduction in duration of hypoglycemia episodes per patient (CGM 44[10-140] min versus IGM 95[15-520] min, p<0.05). Moreover in this brief study of the first three days of life they also found a reduction in the total number of pokes per patient of 5 pokes (22 vs 16). The numbers however are small and the duration short in only being three days so it did not provide a perfect answer as to whether this technology would work in babies from 500-750g reliably but certainly for older babies, continuous knowledge of the blood glucose in theory would allow for faster response to low sugars and as a result as evidenced by the results led to a decrease in time with a low blood glucose.
Improving on these results
Galderisi et al just published Continuous Glucose Monitoring in Very Preterm Infants: A Randomized Controlled Trial. The study remains small at 50 and the target group ranging from 28-31 weeks (all < 1500g) but the study followed babies for a longer time frame of 7 days. This study employed an algorithm for adjustments in glucose infusion that required staff to first put data into an excel spreadsheet and then the predictive algorithm dictated whether to increase or decrease the rate of dextrose infusion. In one arm, CGM results were unblinded and the practitioners relied on the rate of change to determine the predicted glucose 15 minutes into the future while in the blinded group the CGM was used but results were not available (retrospectively yes) so changes were made based on the usual practice of obtaining point of care results and modifying glucose infusion rates based on that result. The primary outcome of interest here was percentage of time in the euglycemic range of 72 – 144 mg/dL (4-8 mmol/L). Secondary outcomes were time spent hypo or hyperglycemic (mild hypoglycemia (M-HYPO) (47–71 mg/dL); severe hypoglycemia (S-HYPO) (<47 mg/dL); mild hyperglycemia (M-HYPER) (145–180 mg/dL); and severe hyperglycemia (S-HYPER) (>180 mg/dL)). The study lasted a total of seven days allowing the use of one subcutaneous probe per patient as they can last one week after insertion.
How did the approaches compare?
As you might have expected, having a predictive model proved superior. Overall after adjusting for sex, gestational age and weight mean time in target using the unblinded CGM was 83% [95% CI, 79%–87%] and of 71% [95% CI, 67%–76%] in B-CGM [P < .001]). 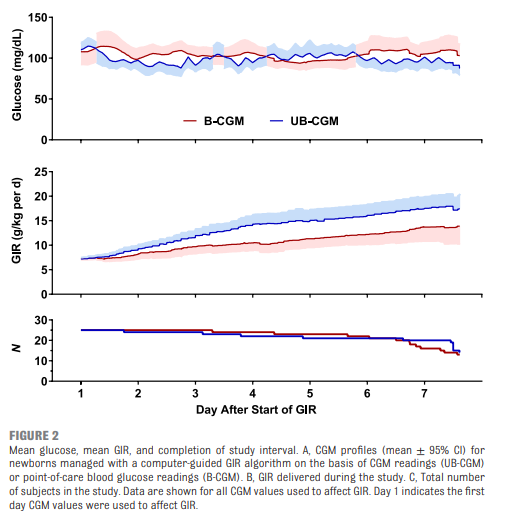

As for secondary outcomes one can see that the time spent in the hypo/hyper areas was much less as a percentage of time than using traditional methods of intermittent sampling. One interesting outcome was that the total number of samples used over the study was an average of 2.4 tests per day in the unblinded group vs 2.59 per day in the intermittent sampling group which although statistically different does not seem to have much clinical impact.
A few questions remain
The idea of using an implanted CGM for infants in the NICU is one that excites me. The lack of a reduction in pokes in a meaningful way is disappointing but I can’t help but wonder if the effect was different whether you were in the first or second half of the week. What if glycemic control in these 29-31 week infants had stabilized by 2-3 days such that you only needed one or two glucose checks in the last half of the week per day? The CGM requires calibration twice daily with POC samples so the lack of a difference my be due to those issues. Future, calibration is rumoured to be possible with one sample so that may change.
There is no disputing though that the use of the predictive algorithm made a difference in terms of avoidance of hypo/hyperglycemic episodes. A larger study would be needed to look at whether this impacts harm that may be associated with such variability such as IVH or ROP but it certainly is promising. The biggest issue here is that I cannot see people manually inputting glucose readings on the CGM into an excel sheet in everyday practice. For this to become widely adopted, a simplified approach to prediction would be required or even better a feedback loop whereby data from the CGM would relay to the infusion pump and rates adjusted automatically (with manual override available).
The use of CGM is coming though and I can’t help but think in the larger babies born to mothers with diabetes there would be a real heal sparing effect with these. Might this be the next study?

by All Things Neonatal | Nov 16, 2017 | Neonatal, Neonatology, preemie, Prematurity
Given that today is world prematurity day it seems fitting to talk about prematurity at the absolute extreme of it.
It has been some time since as a regional program we came to accept that we would offer resuscitation to preterm infants born as early as 23 weeks gestational age. This is perhaps a little later in the game that other centers but it took time to digest the idea that the rate of intact survival was high enough to warrant a trial of resuscitation. This of course is not a unilateral decision but rather a decision arrived at after consultation with the family and interprofessional team. To be sure it is not an easy one. Other centers have argued that resuscitation should be offered to those infants as young as 22 weeks gestational age and data now exists due to enough centres doing so to provide families with some guidance as to expected survival rates and importantly the likelihood of disability. This topic has been covered previously in /2015/09/25/winnipeg-hospital-about-to-start-resuscitating-infants-at-23-weeks/. Why cover this topic again? Well an article on CNN might have something to do with it.
Resuscitating Below 22 weeks
This week as I was perusing the news I came across a rather shocking article on CNN. Born before 22 weeks, ‘most premature’ baby is now thriving.  The article tells the tale of a baby delivered at 21 weeks and 4 days that now as a three year old is reaching appropriate milestones without any significant impairments. It is a story that is filled with inspiration and so I am not mistaken I am delighted for this child and their family that this outcome has occurred. When the lay press latches onto stories like this there is no doubt a great deal of sensationalism to them and in turn that gathers a lot of attention. This in turn is a great thing for media.
The article tells the tale of a baby delivered at 21 weeks and 4 days that now as a three year old is reaching appropriate milestones without any significant impairments. It is a story that is filled with inspiration and so I am not mistaken I am delighted for this child and their family that this outcome has occurred. When the lay press latches onto stories like this there is no doubt a great deal of sensationalism to them and in turn that gathers a lot of attention. This in turn is a great thing for media.
A Few Caveats Though
With the exception of pregnancies conceived through IVF the best dating we have is only good to about +/- 5 days when an early first trimester ultrasound is performed or the date of the last menstrual period is fairly certain. A baby though who is born at 21 weeks + 4 days may in fact be 22 +3 days or even more depending on when the dating was done (second trimester worse). Let’s not take away though from the outcome being this good even at 22 weeks. That is a pretty perfect outcome for this family but the point is that this baby may in fact be older than 21 weeks.
Secondly, there are millions of babies born each year in North America. Some of these infants are born at 22 weeks. How do they fare overall? From the paper by Rysavy et al from 2015 the results are as follows.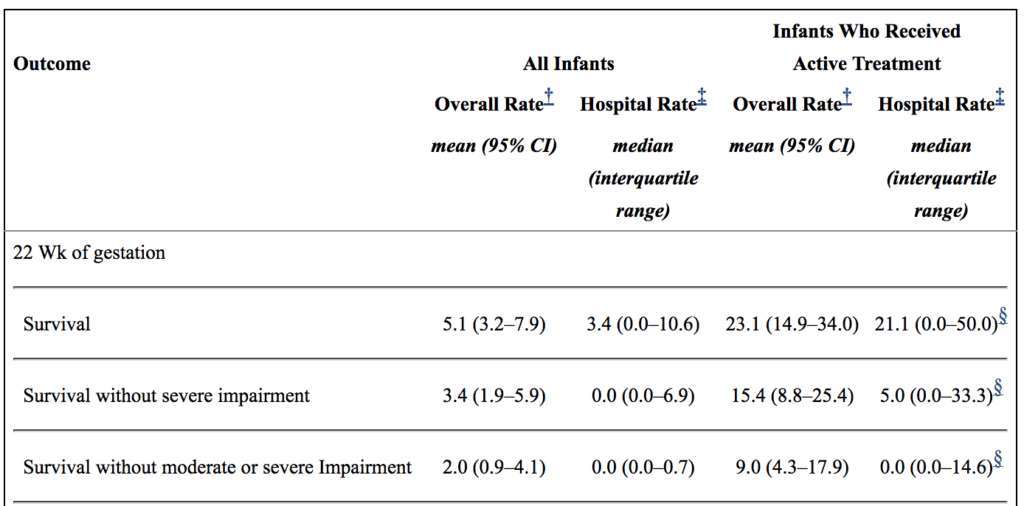
If you look at the overall rate of survival it is on an average of 5.1%. If you take a look though at those infants in whom resuscitation is provided that number increases to a mean of 23%. Intact survival is 9% overall. The odds aren’t great but they are there and I suspect the infant in the article is one of those babies. Flipping the argument though to the glass is half empty, 91% of infants born at 22 weeks by best estimate who are offered resuscitation will have a moderate or severe disability or die. I am not saying what one should do in this situation but depending on how a family processes the data they will either see the 110 chance of intact survival as a good thing or a 9/10 chance of death or disability as a very bad thing. What a family chooses though is anyone’s best guess.
Should we resuscitate below 22 weeks if the family wishes?
I guess in the end this really depends on a couple things. First off, how certain are the dates? If there is any degree of uncertainty then perhaps the answer is yes. If the dates are firm then I at least believe there is a barrier at which futility is reached. Perhaps this isn’t at 21 weeks as some patients may indeed be older but think about what you would offer if a family presented at 20 weeks and wanted everything done. What if it were 19 weeks? I suspect the point of futility for all lies somewhere between 19-21 weeks.
As I prepare to attend the annual meeting in Ottawa tomorrow for the Fetus and Newborn Committee I think it is prudent to point out just how difficult all of this is. The current statement on Counselling and management for anticipated extremely preterm birth I think hits on many of these issues. The statement is the product on not only the think tank that exists on this committee but was the product of a national consultation. I know I may be biased since I sit on the committee but I do believe it really hits the mark.
Should we be thinking about resuscitating at 21 weeks? For me the answer is one clouded by a whole host of variables and not one that can be easily answered here. What I do think though is that the answer in the future may be a yes provided such infants can be put onto an artificial placenta.  Even getting a few more weeks of growth before aerating those lungs is necessary may make all the difference. The NICUs of tomorrow certainly may look quite different than they do now.
Even getting a few more weeks of growth before aerating those lungs is necessary may make all the difference. The NICUs of tomorrow certainly may look quite different than they do now.

by All Things Neonatal | Nov 8, 2017 | Neonatal, neonatal abstinence, Neonatology
It would seem that the Opioid crisis is continuing to be front and centre in the news. Just today the President of the United States declared an Opioid Epidemic Emergency. Of course he was speaking primarily about the damage these drugs do on the family unit and those around them, the impact on the unborn child is significant as well. If this sounds familiar it is because I have written about this topic recently and in the past in the posts A Magic Bullet to Reduce Duration of Treatment and Hospital Stays for Newborns With NAS and Mandatory Drug-Testing ni PRegnancy: Lesson learned. I suppose I write about this topic often as at least where I work this is a problem which just won’t go away and takes up a tremendous amount of resources.
What Can a Large Data Set Tell us?
Pediatrix medical group that you may well be familiar with has a lot of data that can be mined from the hospitals in their network. When it comes to buprenorphine there is a lot of data to look at. In this case the question posed by VN Tolia et al in thier paper Antenatal methadone vs buprenorphine exposure and length of hospital stay in infants admitted to the intensive care unit with neonatal abstinence syndrome was whether there is a difference in infants born to mothers who have been exposed to methadone vs burprenorphine. Specifically they chose to use length of stay as the primary outcome in a retrospective review of 3364 infants admitted for management of NAS. Of these infants, 2202 (65%) were exposed to methadone and 1162 (34%) to buprenorphine. Before we get into what the results actually were it is important to highlight what this study will not tell us. By looking only at admissions for NAS we do not know whether the use of buprenorphine in mothers actually reduced admission for NAS so we are only speaking of the babies who were afflicted with NAS.
When looking at the two groups, the median length of stay was 24 days for the methadone group and 21 for the buprenorphine which was found to be significantly different. In the secondary analysis another interesting finding (at least to me) was noted.
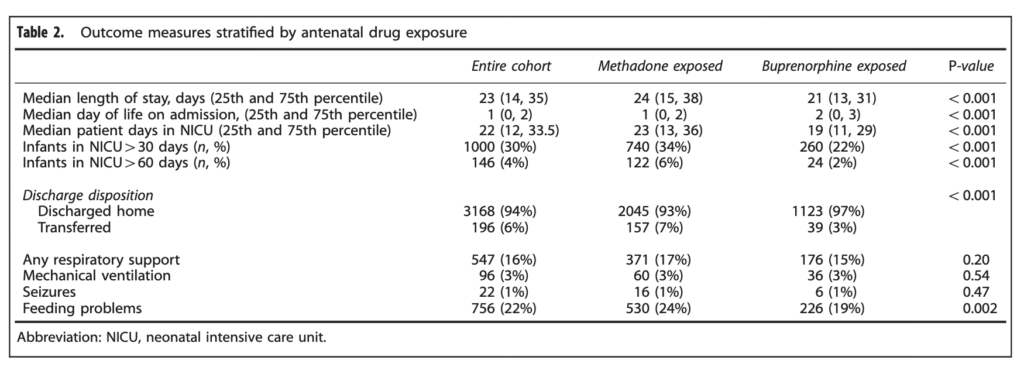 When looking at the percentage of babies with a length of stay > 30 days the difference was significant at 34% vs 22% for buprenorphine. The authors here did a good job of doing their best to control for factors which could have influenced the results as they did a regression analysis to determine whether other factors such as gestational age, sex, type of treatment provided etc would explain the shortened length of stay and they found that it remained significant controlling for a wide variety of factors.
When looking at the percentage of babies with a length of stay > 30 days the difference was significant at 34% vs 22% for buprenorphine. The authors here did a good job of doing their best to control for factors which could have influenced the results as they did a regression analysis to determine whether other factors such as gestational age, sex, type of treatment provided etc would explain the shortened length of stay and they found that it remained significant controlling for a wide variety of factors.
Is three days worth it?
It would be tempting to look at the 3 day median difference and shrug it off as no big deal. Remember though that we are in an epidemic are we not? What the study does not account for as well are the number of babies who could have been managed in a postpartum ward and also had a shortened length of stay. Let’s look at a city though where about 100 babies are admitted a year with NAS. A three day reduction in length of stay would translate into 300 patient days per year. By simply changing the medication a woman is being treated with in pregnancy from methadone to buprenorphine we could save almost one NICU bed for the whole year. That is nothing to sneeze at! Moreover if the reduction in admission rates are also true another one, two or more beds per year could be spared depending on the effectiveness of the drug.
In the last post that spoke of using buprenorphine to treat NAS in babies I was concerned about the alcohol content of the syrup for administration in babies. Here we are talking about treating women rather than babies so this is not a concern (plus they would not be taking the pediatric suspension). I see little downside to using buprenorphine over methadone so the real question is how do we get the care providers for the mothers to make the switch? I have a feeling that is coming sooner rather than later.
