I had the pleasure of meeting the author of a paper I am about to comment on this week while at the 99 NICU conference in Stockholm. Dr. Ohlin from Orebro University in Sweden presented very interesting work on their unit’s “scrub the hub” campaign. As he pointed out, many places attempt to reduce coagulase negative staphylococcal infections by introducing central line bundles but seldom is there one thing that is changed in a bundle that allows for a before and after comparison like his team was able to do. I was so impressed by this work and at the same time concerned about another strategy to reduce infection that I felt compelled to make a comment here.
Scrub the hub!
Dr. Ohlin and the first author Dr. Bjorkman published Scrubbing the hub of intravenous catheters with an alcohol wipe for 15 sec reduced neonatal sepsis back in 2015. They compared a 16.5 month period in their unit when they rolled out a CLABI reduction bundle to a period of 8.5 months afterwards when they made one change. Nurses as is done in the units I work in were commonly scrubbing the hub before they injected the line with a medication but in the second epoch the standard changed to be a specified 15 second scrub instead of being left up to the individual nurse. With permission from Dr. Ohlin here is a picture of the hubs highlighting bacterial growth without scrubbing, then for a duration less than 15 seconds and then with 15 seconds.
In the first epoch they had 9 confirmed CLABSIs and 0 confirmed in the second after their intervention. The rate of CLABSI then in the first epoch was 1.5% vs 0% in the second group. As with any study looking at sepsis, definitions are important and while they didn’t do paired cultures to rule out contamination (one positive and one negative as is the definition in our hospitals) they did refer each patient to a senior Neonatologist to help determine whether each case should be considered a true positive or not. Given that they made no changes to practice or other definitions in diagnosing infections during that time perhaps the results were indeed real. Presumably if they had missed an infection and not treated it in the second epoch the patient would have declared themselves so I think it is reasonable to say that 8.5 months without a CLABSI after their intervention is a success. As Dr. Ohlin points out the scrub duration may also help due to the abrasion of the hub surface removing a bacterial film. Regardless of the reason, perhaps a 15 second scrub is a good idea for all?
The lazy person’s solution – the SwabCap
One way to get around human nature or people being distracted might be to cover each luer lock with a cap containing 70% isopropyl alcohol. In this way when you go to access the line there should be no bacteria or labour required to scrub anything since the entry of the line is bathed in alcohol already. This was the subject of a systematic review from the Netherlands entitled Antiseptic barrier cap effective in reducing central line-associated bloodstream infections: A systematic review and meta-analysis. The reviews ultimately examined 9 articles that met their inclusion criteria and found the following; use of the antiseptic barrier cap was effective in reducing CLABSIs (IRR = 0.59, 95% CI = 0.45–0.77, P < 0.001). Moreover, they concluded that this was an intervention worth adding to central-line maintenance bundles. Having said that, the studies were mostly adult and therefore the question of whether minute quantities of isopropyl alcohol might be injected with medications was not a concern when they made their conclusion.
What about using such caps in ELBW infants
Sauron et al in St. Justine Hospital in Montreal chose to look at these caps more carefully after they were implemented in their NICU. The reason for taking a look at them was due to several luer valves malfunctioning. The authors created an in-vitro model to answer this question by creating a closed system in which they could put a cap on the end of a line with a luer lock and then inject a flush, followed by a simulated medication (saline) and then a flush and collect the injected materials in a glass vial that was sealed to prevent evaporative loss of any isopropyl alcohol. They further estimated the safe amount of isopropyl alcohol from Pediatric studies would be 1% of the critical threshold of this alcohol and using a 500g infant’s volume of distribution came up with a threshold of 14 mmol/L. The study then compared using the SwabCap over two different valve leur lock systems they had in their units (SmartSite and CARESITE valves) vs. using the strategy of “scrub the hub”.
The results were quite concerning and are shown below.
Circuit Type
Temperature
Sample 1
Sample 2
Sample 3
Mean
SwabCap on Smart Site Valve
Room
49.5
58.4
46.8
51.6
Incubator 35 degrees
45.16
94.7
77.9
72.6
SwabCap on CARESITE valve
Room
14.1
5.7
5.2
8.34
Incubator 35 degrees
7.0
8.1
5.9
7.0
Isopropyl alcohol pad on CARESITE Valve
Room
0
0
0
0
Certainly, the Smart Site valve allowed considerable amounts of isopropyl alcohol to enter the line but the CARESITE while better still allowed entry compared to the control arm which allowed none. Beyond the introduction of the alcohol into the system in all cases considerable clouding of the valves occurred with repeated capping of the system with new caps as was done with each med injection since each was single use. In lines that were not accessed contact with the cap was left for 96 hours as per recommendations from the manufacturer and these changes occurred as well.
Conclusion
While a reduction in CLABSI is something we all need to strive to obtain, it is better to take the more difficult path and “scrub the hub” and by that for 15 seconds which incidentally is the same recommended duration for hand hygiene in both of our units. Perhaps in larger term infant’s seepage of isopropyl alcohol into the lines would not be as concerning as their larger volume of distribution would lead to lower levels but I would ask the question “should any isopropyl alcohol be injected into any baby?”. I think not and perhaps by reading this post you will ask the same thing if your unit is using these caps.
Thank you to Örebro University Hospital for their permission in using the photo for the post
Look around you. Technology is increasingly becoming pervasive in our everyday lives both at home and at work. The promise of technology in the home is to make our lives easier. Automating tasks such as when the lights turn on or what music plays while you eat dinner (all scripted) are offered by several competitors. In the workplace, technology offers hopes of reducing medical error and thereby enhancing safety and accuracy of patient care. The electronic health record while being a nuisance to some does offer protection against incorrect order writing since the algorithms embedded in the software warn you any time you stray. What follows is a bit of a story if you will of an emerging technology that has caught my eye and starts like many tales as a creative idea for one purpose that may actually have benefits in other situations.
Meet Stethocloud
In 2012 students in Australia rose to the challenge and designed a digital stethoscope that could be paired with a smartphone. The stethoscope was able to send the audio it was receiving to the smartphone for analysis and provide an interpretation. The goal here was to help diagnose childhood pneumonia with a stethoscope that would be affordable to the masses, even “Dr. Mom” as the following video documents. Imagine before calling your health line in your city having this $20 tool in your hands that had already told you your child had breath sounds compatible with pneumonia. Might help with moving you up the triage queue in your local emergency department.
Shifting the goal to helping with newborns
Of course breath sounds are not the only audio captured in a stethoscope. Heart sounds are captured as well and the speed of the beats could offer another method of confirming the heart is actually beating. Now we have ECG, pulse oximetry, auscultation and palpation of the umbilical stump to utilize as well so why do you need another tool? It comes down to accuracy. When our own heart rates are running high, how confident are we in what we feel at the stump (is that our own pulse we are feeling?). In a review on measurement of HR by Phillipos E et al from Edmonton, Alberta, auscultation was found to take an average of 17 seconds to produce a number and in 1/3 of situations was incorrect. The error in many cases would have led to changes in management during resuscitation. Palpation of the umbilical cord is far worse. In one study “cord pulsations were impalpable at the time of assessment in 5 (19%) infants, and clinical assessment underestimated the ECG HR with a mean (SD) difference between auscultation and palpation and ECG HR of − 14 (21) and − 21 (21) beats min –1″. In another study, 55% of the time providers were incorrect when they thought the HR was under 100 BPM. This leaves the door open for something else. Might that something be the digital stethoscope?
How does the digital stethoscope fare?
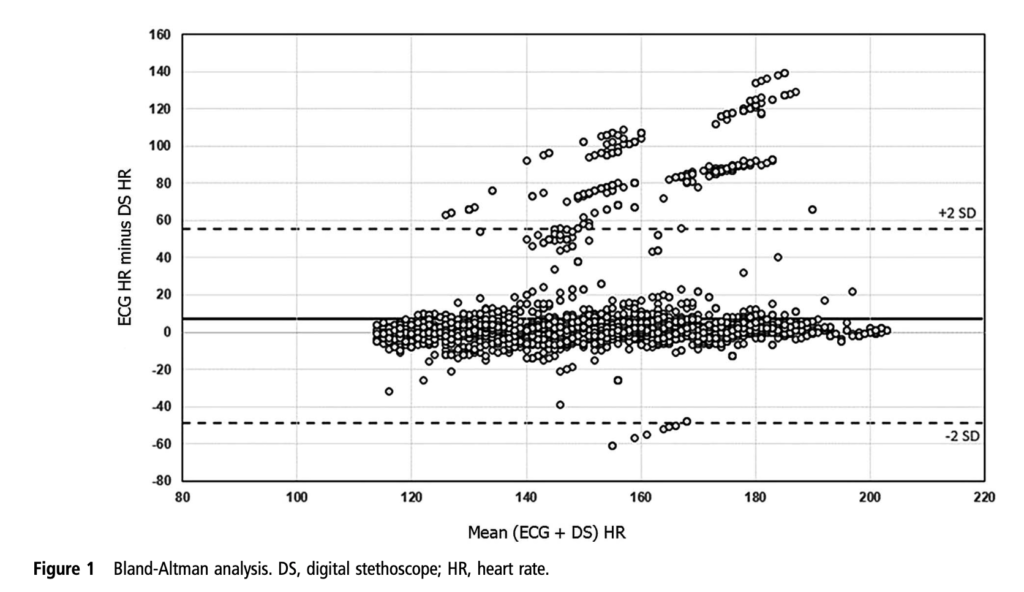
Kevac AC et al decided to look at the use of the Stethocloud to measure HR after birth in infants >26 weeks gestational age at birth. The opted to use the ECG leads as the gold standard which arguably is the most accurate method we have for detecting HR. The good news was that the time to signal acquisition was pretty impressive. The median time to first heart rate with the stethoscope was 2 secs (IQR 1-7 seconds). In comparison the time for a pulse oximeter to pick up HR is variable but may be as long as one minute. In low perfusion states it may be even longer or unable to pick up a good signal. The bad news was the accuracy as shown in the Bland Altman plot. The tendency of the stethoscope was to underestimate the EKG HR by about 7 BPM. Two standard deviations though had it underestimate by almost 60 BPM or overestimate by about 50 BPM. For the purposes of resuscitation, this range is far to great. The mean is acceptable but the precision around that mean is to wide. The other issue noted was the frequent missing data from loss of contact with the patient. Could you imagine for example having a baby who has a heart rate of 50 by the stethoscope but by EKG 100? Big difference in approach, especially if you didn’t have EKG leads on to confirm. The authors note that the accuracy is not sufficient and felt that an improvement in the software algorithms might help.
Another go at it
So as suggested, the same group after having a new version with improved software decided to go at it again. This time Gaertner VD et al restricted the study to term infants. Forty four infants went through the same process again with the stethoscope output being compared to EKG lead results. This time around the results are far more impressive. There was virtually no difference between the ECG and the stethoscope with a 95% confidence interval as shown in the graphs with A being for all recordings and B being those without crying (which would interfere with the acquiring of HR). A maximal difference of +/- 18 BPM for all infants is better than what one gets with auscultation or palpation in terms of accuracy and let’s not forget the 2 second acquisition time!
Should you buy one?
I think this story is evolving and it wouldn’t surprise me if we do see something like this in our future. It certainly removes the element of human error from measuring. It is faster to get a signal than even the time it takes to get your leads on. Where I think it may have a role though is for the patient who has truly no pulse. In such a case you can have an EKG HR but the patient could be in pulseless electrical activity. Typically in this case people struggle to feel a pulse with the accuracy being poor in such situations. Using a device that relies on an actual heart contraction to make a sound provides the team with real information. Concurrent with this technology is also the rise of point of care ultrasound which could look at actual cardiac contractions but this requires training that makes it less generalizable. Putting a stethoscope on a chest is something we all learn to do regardless of our training background.
I think they could be on to something here but perhaps a little more evidence and in particular a study in the preterm infant would be helpful to demonstrate similar accuracy.
I don’t envy our nurses who care for babies withdrawing from various opiates and other substances. These assignments are definitely a challenge and require a great deal of patience and depending on the shrillness of an infant’s cry a good set of earplugs. Nonetheless we do our best with these infants to keep them calm and avoid as much stimulation as we can as we attempt to minimize the excitability of their nervous system.
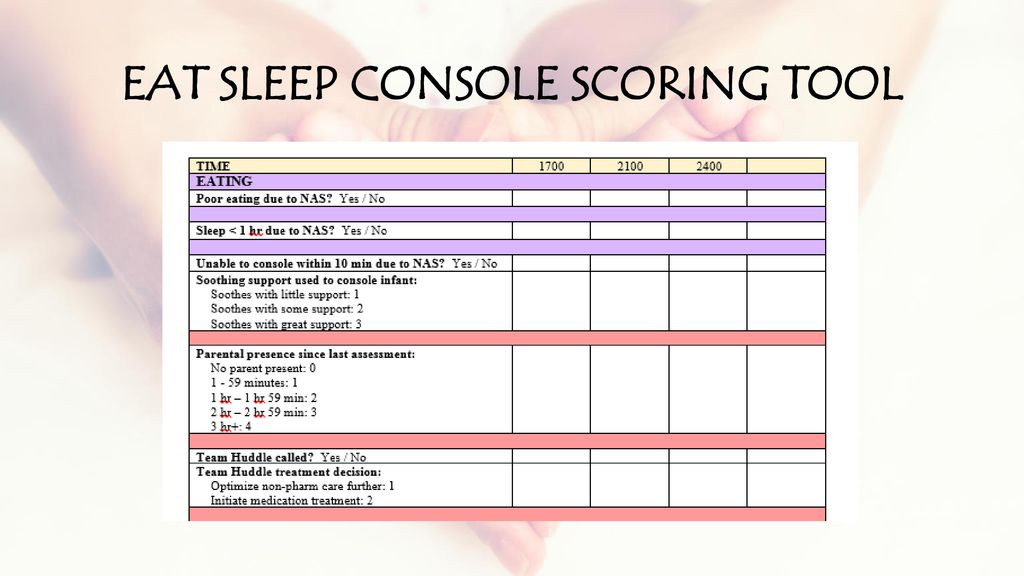
Over 40 years ago the Finnegan Neonatal Abstinence scoring system was developed to assist medical teams by providing as objective a system as possible to compare one infant to another and determine when and if a patient should be treated pharmacologically. Unfortunately there is a problem inherent with this scoring system. It is the same problem that exists when you don’t have a blinded research trial. Imagine you are caring for an infant and you were given no history about drug exposure. How might you score a patient like that compared to one in which you are told has been exposed to illicit substances? Your senses are heightened and moreover if you were told this baby is “withdrawing terribly” or “is awful at night” you are biased. How are you likely to score such a patient when they are “on the edge” of being counted as a 1 or a 0 in a category? I bet in many cases, especially if you haven’t taken care of many such patients you err on the side of caution and score them on the high side. It is human nature. When the possible outcome of failing to recognize a withdrawing patient is a seizure, no one wants to be on when it happens having their scoring questioned. Have a look at the scoring tool though.
There is a lot of stuff in there to check off! What if it could be simpler?
The ESC Tool
In early May, news began to break of an abstract being presented at the Pediatric Academic Society meeting. The news story from the AAP can be found here. The ESC tool is a three question tool used to assess whether an infant requires treatment for withdrawal.
E – Eat (is an infant is able to eat 1 or more ounce per feeding)
S – Sleeping (sleep for an hour or longer undisturbed)
C – Console (Be consoled in 10 minutes or less.)
If all three criteria are met, the patient does not need treatment. If one or more criteria are not met the housestaff are notified and first non-pharmacologic and then pharmacologic means are employed if necessary to control symptoms.
The authors did something quite interesting. They looked at 50 patients with 201 hospital days with prenatal exposures to opiates and applied the ESC criteria to guide treatment. Concurrently they captured the Finnegan scores but did not use them to guide treatment.
The findings I hope you will agree are quite interesting!
“FNASS scores indicated starting morphine in 30 infants (60%). Morphine was actually started on only 6 patients (12%) (p< 0.0001) based on the ESC approach. The FNASS led protocol directed initiating or increasing meds on 24.6% of days compared to 2.7% of days using the ESC approach (p< 0.0001). The FNASS approach directed that morphine was either not started or decreased on 65.8% of days compared with 94.4% of days using the ESC approach (p< 0.0001). There were no readmissions or reported adverse events.
Pretty amazing but…
The ESC approach greatly reduced the need for treatment and as the authors state there were no readmissions or reported adverse events. What we don’t know and will be needed I suspect before anyone will adopt this strategy (which I have to say again is so much simpler that current approaches) is how these children do in the long run. If the system is undertreating withdrawal, could we see downstream impacts of a “kinder and gentler” approach? One outcome that will be reported soon in the next month is length of stay. I am eagerly awaiting further results as I for one think that a simpler approach to these patients may be just what the doctor ordered. I think the nurses might thank us as well but we will see just how appropriate it is!
The Abstract reporting these findings can be found below
If there is one thing that keeps coming back as a lesson again and again in life it is the importance of communication. Whether it be in the home or at work, too many of our “problems” in the workplace come down to whether or not our teams talk to one another effectively.
A tremendous source of stress of course is the unknown. When a baby is born in the field we can only rely on the information being presented to us via telephone contact. In the melee that occurs on arrival of a potentially sick patient, details can be missed.
The following video illustrates such a situation and I believe aptly provides a good example of how to communicate in such a way that the stress of the situation is relieved. If we can all strive to slow things down just a little we may find that communication eliminates much of the tension in such a situation.
If you are looking to “slow” down your life and improve things such as communication style you may want to have a look at the book “In Praise of Slow” as we head into the weekend. It’s all about slowing things down to actually improve efficiency. The world is moving pretty quickly these days and couldn’t we all do with a little more efficiency and less wasted time? In Neonatology we are confronted with surprises every day, often with little notice. If we can slow things down and pass on the needed information to the right people at the right time we will help to reduce errors if we can just get it right the first time!
As you can tell I am a big fan of simulation in helping to create high functioning teams! More of these videos can be accessed on my Youtube channel at


 decided to look at the use of the Stethocloud to measure HR after birth in infants >26 weeks gestational age at birth. The opted to use the ECG leads as the gold standard which arguably is the most accurate method we have for detecting HR. The good news was that the time to signal acquisition was pretty impressive. The median time to first heart rate with the stethoscope was 2 secs (IQR 1-7 seconds). In comparison the time for a pulse oximeter to pick up HR is variable but may be as long as one minute. In low perfusion states it may be even longer or unable to pick up a good signal. The bad news was the accuracy as shown in the Bland Altman plot. The tendency of the stethoscope was to underestimate the EKG HR by about 7 BPM. Two standard deviations though had it underestimate by almost 60 BPM or overestimate by about 50 BPM. For the purposes of resuscitation, this range is far to great. The mean is acceptable but the precision around that mean is to wide. The other issue noted was the frequent missing data from loss of contact with the patient. Could you imagine for example having a baby who has a heart rate of 50 by the stethoscope but by EKG 100? Big difference in approach, especially if you didn’t have EKG leads on to confirm. The authors note that the accuracy is not sufficient and felt that an improvement in the software algorithms might help.
decided to look at the use of the Stethocloud to measure HR after birth in infants >26 weeks gestational age at birth. The opted to use the ECG leads as the gold standard which arguably is the most accurate method we have for detecting HR. The good news was that the time to signal acquisition was pretty impressive. The median time to first heart rate with the stethoscope was 2 secs (IQR 1-7 seconds). In comparison the time for a pulse oximeter to pick up HR is variable but may be as long as one minute. In low perfusion states it may be even longer or unable to pick up a good signal. The bad news was the accuracy as shown in the Bland Altman plot. The tendency of the stethoscope was to underestimate the EKG HR by about 7 BPM. Two standard deviations though had it underestimate by almost 60 BPM or overestimate by about 50 BPM. For the purposes of resuscitation, this range is far to great. The mean is acceptable but the precision around that mean is to wide. The other issue noted was the frequent missing data from loss of contact with the patient. Could you imagine for example having a baby who has a heart rate of 50 by the stethoscope but by EKG 100? Big difference in approach, especially if you didn’t have EKG leads on to confirm. The authors note that the accuracy is not sufficient and felt that an improvement in the software algorithms might help. There was virtually no difference between the ECG and the stethoscope with a 95% confidence interval as shown in the graphs with A being for all recordings and B being those without crying (which would interfere with the acquiring of HR). A maximal difference of +/- 18 BPM for all infants is better than what one gets with auscultation or palpation in terms of accuracy and let’s not forget the 2 second acquisition time!
There was virtually no difference between the ECG and the stethoscope with a 95% confidence interval as shown in the graphs with A being for all recordings and B being those without crying (which would interfere with the acquiring of HR). A maximal difference of +/- 18 BPM for all infants is better than what one gets with auscultation or palpation in terms of accuracy and let’s not forget the 2 second acquisition time!
 If you are looking to “slow” down your life and improve things such as communication style you may want to have a look at the book “In Praise of Slow” as we head into the weekend. It’s all about slowing things down to actually improve efficiency. The world is moving pretty quickly these days and couldn’t we all do with a little more efficiency and less wasted time? In Neonatology we are confronted with surprises every day, often with little notice. If we can slow things down and pass on the needed information to the right people at the right time we will help to reduce errors if we can just get it right the first time!
If you are looking to “slow” down your life and improve things such as communication style you may want to have a look at the book “In Praise of Slow” as we head into the weekend. It’s all about slowing things down to actually improve efficiency. The world is moving pretty quickly these days and couldn’t we all do with a little more efficiency and less wasted time? In Neonatology we are confronted with surprises every day, often with little notice. If we can slow things down and pass on the needed information to the right people at the right time we will help to reduce errors if we can just get it right the first time!