

A strange title perhaps but not when you consider that both are in much need of increasing muscle mass. Muscle takes protein to build and a global market exists in the adult world to achieve this goal. For the preterm infant human milk fortifiers provide added protein and when the amounts remain suboptimal there are either powdered or liquid protein fortifiers that can be added to the strategy to achieve growth. When it comes to the preterm infant we rely on nutritional science to guide us. How much is enough? The European Society For Pediatric Gastroenterology, Hepatology and Nutrition published recommendations in 2010 based on consensus and concluded:
“We therefore recommend aiming at 4.0 to 4.5 g/kg/day protein intake for infants up to 1000 g, and 3.5 to 4.0 g/kg/day for infants from 1000 to 1800 g that will meet the needs of most preterm infants. Protein intake can be reduced towards discharge if the infant’s growth pattern allows for this. The recommended range of protein intake is therefore 3.5 to 4.5 g/kg/day.”
These recommendations are from six years ago though and are based on evidence that preceded their working group so one would hope that the evidence still supports such practice. It may not be as concrete though as one would hope.
Let’s Jump To 2012
Miller et al published an RCT on the subject entitled Effect of increasing protein content of human milk fortifier on growth in preterm infants born at <31 wk gestation: a randomized controlled trial. This trial is quite relevant in that it involved 92 infants (mean GA 27-28 weeks and about 1000g on average at the start), 43 of whom received a standard amount of protein 3.6 g/kg/day vs 4.2 g/kg/d in the high protein group. This was commenced once fortification was started and carried through till discharge with energy intakes and volume of feeds being the same in both groups. The authors used a milk analyzer to ensure consistency in the total content of nutrition given the known variability in human milk nutritional content. The results didn’t show much to write home about. There were no differences in weight gain or any measurements but the weight at discharge was a little higher in the high protein group. The length of stay trended towards a higher number of days in the high protein group so that may account for some of the difference. All in all though 3.6 or 4.2 g/kg/d of protein didn’t seem to do much to enhance growth.
Now let’s jump to 2016
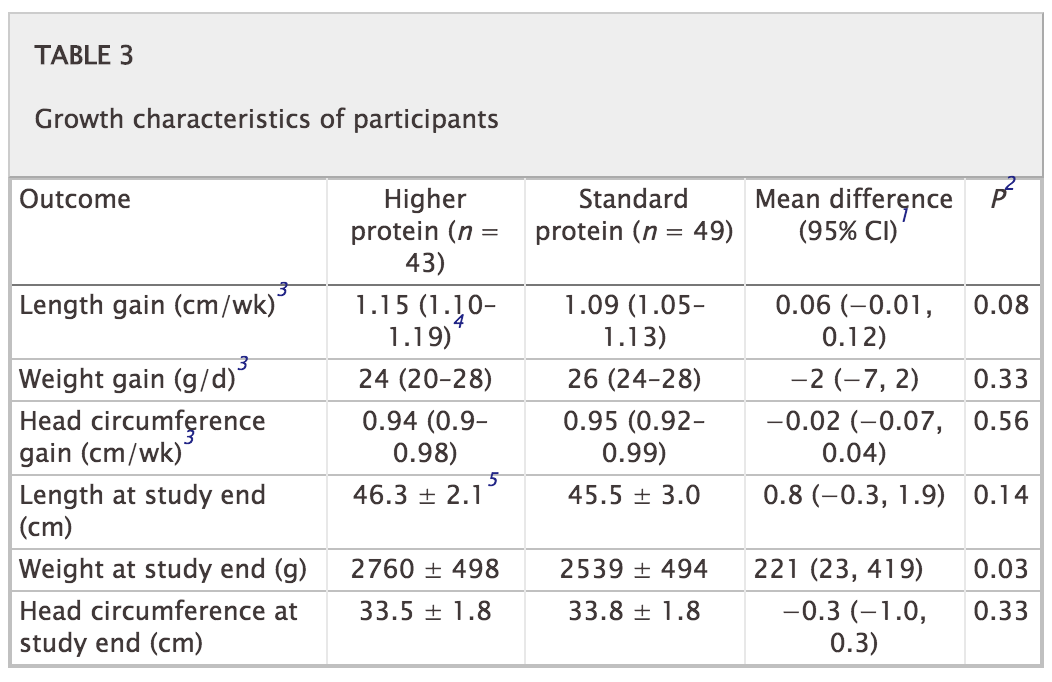
This past month Maas C et al published an interesting trial on protein supplementation entitled Effect of Increased Enteral Protein Intake on Growth in Human Milk-Fed Preterm Infants: A Randomized Clinical Trial. This modern day study had an interesting question to answer. How would growth compare if infants who were fed human milk were supplemented with one of three protein contents based on current recommendations. The first group of 30 infants all < 32 weeks received standard protein intake of 3.5 g/kg/d while the second group of 30 were given an average intake of 4.1 g/kg/d. The second group of 30 were divided though into an empiric group in which the protein content of maternal or donor milk was assumed to be a standard amount while the second 15 had their protein additive customized based on an analysis of the human milk being provided. Whether the higher intake group was estimated or customized resulted in no difference in protein intake on average although variability between infants in actual intake was reduced. Importantly, energy intake was no different between the high and low groups so if any difference in growth was found it would presumably be related to the added protein.
Does it make a difference?
The results of this study failed to show any benefit to head circumference, length or weight between the two groups. The authors in their discussion postulate that there is a ceiling effect when it comes to protein and I would tend to agree. There is no question that if one removes protein from the diet an infant cannot grow as they would begin to break down muscle to survive. At some point the minimum threshold is met and as one increases protein and energy intake desired growth rates ensue. What this study suggests though is that there comes a point where more protein does not equal more growth. It is possible to increase energy intakes further as well but then we run the risk of increasing adiposity in these patients.
I suppose it would be a good time to express what I am not saying! Protein is needed for the growing preterm infant so I am not jumping on the bandwagon of suggesting that we should question the use of protein fortification. I believe though that the “ceiling” for protein use lies somewhere between 3.5 – 4 g/kg/d of protein intake. We don’t really know if it is at 3.5, 3.7, 3.8 or 3.9 but it likely is sitting somewhere in those numbers. It seems reasonable to me to aim for this range but follow urea (something outside of renal failure I have personally not paid much attention to). If the urea begins rising at a higher protein intake approaching 4 g/kg/d perhaps that is the bodies way of saying enough!
Lastly this study also raises a question in my mind about the utility of milk analyzers. At least for protein content knowing precisely how much is in breastmilk may not be that important in the end. Then again that raises the whole question of the accuracy of such devices but I imagine that could be the source of a post for another day.
And history keeps repeating itself. Stan Zlotkin in HSC, TO, found a ceiling for protein intake as well, FORTY years ago. Granted, the prems weren’t as small then (not under 1,200g) as they are today. Thanks for the summary.