Like many Neonatologists, I experience a complete body sigh when I discover that an ELBW infant has a PDA. Once I find out that once again another duct has reared it’s ugly head so to speak a number of thoughts run through my head. Should I treat it? With what? For how long? What if the first treatment doesn’t work? Should I have given prophylactic indomethacin? If I do that how any ELBWs will experience significant renal impairment or worse NEC based on that decision? Then we move into a completely different territory that occurs after the duct has been unsuccessfully treated. To ligate or not to ligate? With so many questions and so many conflicting papers in the literature some of which say the ductus is associated but not causative for this or that outcome it is no wonder I am still largely in the dark as to what is truly the best approach.
What about prophylactic indomethacin?
With respect to the use of prophylactic indomethacin the TIPP study clearly showed that while units could reduce the incidence of PDA and with in severe intraventricular hemorrhage the impact on neurodevelopment was unchanged. This was definitely unfortunate news as the trade off then to exposing all of the infants < 1000g in a unit to an increased risk of renal impairment and NEC would not be seemingly worth it. As PDAs are found more commonly in those ELBWs who are not exposed to antenatal steroids, a 2011 paper questioned whether provision of indomethacin prophylaxis only to those babies without steroids was published. Unfortunately the results were not as hoped as no benefit to this subgroup was noted.
Ibuprofen has been associated with less renal impairment and lower risk of NEC but unfortunately we do not have any long term outcome results from ELBWs treated with such therapy. It is promising though that the Cochrane review on the subject found a number of positive short term outcomes from the use of such treatment. In 7 studies included the rates of development of a PDA, repeat courses of NSAIDs and surgical ligations were all reduced with this therapy.
More recently several papers studying paracetamol (tylenol) as a medicine to promote ductal closure have been published but results have been mixed and the lack of large RCTs make it difficult to advocate for it’s regular use instead of ibuprofen or indomethacin. A cochrane review comparing oral ibuprofen to oral paracetamol has been published in 2015 and does show based on the two studies included that the drugs are likely equally efficacious in closing a ductus with an added benefit of paracetamol being less oxygen usage and hyperbilirubinemia compared to ibuprofen. Recent data in mice however linking autism to fetal exposure to paracetamol has necessitated longer term outcome data before this treatment can be recommended instead of the current ibuprofen or indomethacin.
What about the option of benign neglect?
Another option exists however which is to manage any symptoms resulting from the PDA and allow it to close on it’s own. This was the subject of a recent paper published in Archives of Diseases and Childhood Fetal and Neonatal Ed by Rolland et al. The authors of this study describe their experience retrospectively during a time in which there was intentional avoidance of treatment of any kind including ligation for the ductus. What this allows for is a comprehensive assessment of the natural history of the ductus in their cohort of 103 infants between 24-27 weeks gestational age.
Although the study began with 103 infants there were 12 infants (12% of the cohort) that died prior to 72 hours which was the time when the identification of the PDA would have been done. We do not know if these infants died from the PDA or not but it is fair to agree with the authors that unless prophylactic indomethacin was being used this outcome would not have been avoidable. Looking at the remainder of the group, 8 were found to have no PDA at 72 hours while an additional 13 had either no ECHO (10) or died (3) so were not followed. In the ten cases that did not have an ECHO the reason was the lack of respiratory support so presumably the ECHO result would have been irrrelevant to care. The remaining 70 are described in the following table where HNSPDA is a hemodynamically non significant PDA, HSPDA refers to a significant PDA and IDHS means insufficient data on the hemodynamic status although the PDA is still there.
HNSPDA (n=30)
HSPDA (N=23)
IDHS (N=17)
Spontaneous closure
22 (73)
18 (78)
11 (65)
Death before discharge
4 (13)
2 (9)
5 (29)
Survival at discharge with a PDA
4 (13)
2 (9)
1 (6)
Ligation of PDA
0
1 (4)
0
The paper is intriguing for a number of reasons. The first is that by an average age of two months 73% of the PDAs closed from the 70 patients that had documented persistence after 72 hours. We know that from the group of 91, 8 had closure at 72 hours which leaves 83 with a PDA. An additional 10 were not studied as mentioned above as they had no symptoms so we can assume they did not have a HSPDA. Of the three that died however we do not know if the PDA contributed. Looking at the 70 patients left 11 more patients died and 7 were discharged with a PDA. The authors do not disclose the fate of those additional 7. Did they have a ligation after discharge or not and by what method? If they were ligated this is still a positive outcome inn my my mind as the larger infant at that point would likely tolerate a surgical or catheter based closure much better with less morbidity.
It can also not be ignored that in this study the incidence of pulmonary hemorrhage was high at 25% and severe IVH in 21%. Both of these outcomes may be affected by the presence of a PDA so one important question raised here is an ethical one. Clearly many of the children studied who were not treated avoided complications related to treatment which is a good thing. The concern however is that by not treating there may have been excessive morbidity in those who developed the above complications and lacking from the study is follow-up of the survivors to see if their outcome. We also clearly don’t know what the PDA may have contributed to death in this study which is also clearly an important outcome to consider.
I wish I could give you the answer of what to do with these kids. Watch and wait or treat? I suspect in the end we will likely settle on a hybrid approach guided by information gleaned from Targeted Neonatal Echocardiography as was discussed in a post on the topic which can be found here. I think the future state will likely see us using a strategy of selecting some infants by risk categorization to receive prophylactic indomethacin, some to have TNE done between 48 – 72 hours with or without the use of biomarkers to identify those who are likely to get a HSPDA and then treat those and then a final group that we may watch.
What the above study adds to the literature though is that in this final category who we may watch and wait there is about a 75% chance that they will close on their own. If we can pick out the ones that are not HSPDA I suspect the spontaneous closure rate would be even higher. While I am grateful for the publication of this article for now I will continue to pick and choose as best I can which ducts we need to deal with and those we don’t. Hopefully with time and more knowledge my body sighs will be replaced by a look of confidence as I explain to families what is needed for their child.
I was asked to see a woman carrying a fetus this week who was not yet 21 weeks. It was to be honest a very unusual consult as she was clearly pre-viable to me and this was only the second time in my career that I had been asked to do so before 22 or 23 weeks. In the course of our conversation she said the following:
“I know I just have to get to 22 weeks. Everyone knows that at St. Boniface Hospital they are saving kids at 22 weeks now and they will try to resuscitate mine if I can just get a little longer out of this pregnancy”
You might think I was shocked to hear this but I wasn’t as I had warned a group of health professionals ironically minutes earlier that we were going to start hearing things like this due to misinterpretations of both the medical literature and mainstream media. When I asked her where she heard this, her response was that everyone at the clinic she goes to are talking about it. I can only wonder how many other clinics, mom’s groups, Twitter and Facebook posts are saying the same thing! I spent some time with her and provided her with my view on the topic and we agreed not to do anything for her infant until they were bigger (currently was under 300g) and at least 22 5/7 weeks. I am not saying I necessarily believe we should strongly go for an infant at 22 5/7 weeks but she is right that we have and if taking in all the information she wants us to try, now that the public is aware how can we not?
Before I go on let me be clear about the actual state in our city at the moment:
WE ARE NOT RECOMMENDING RESUSCITATION OF ALL INFANTS AT 22 WEEKS OR EVEN 23 WEEKS BUT ARE HAVING DISCUSSIONS ABOUT 23 WEEKS
One Article Causes A Great Stir
In late April the New England Journal of Medicine published an article entitled Between-Hospital Variation in Treatment and Outcomes in Extremely Preterm Infants. What followed were numerous media articles about infants born at 22 or 23 weeks discussing the pros and cons of such actions. Furthermore an explosion of testimonies from parents who had infants resuscitated with good outcomes at these gestational ages ensued. Given that this topic was a hot one and in the public eye, our own local health news agency got in on the action and published the following story called Meet Mac: one of the youngest babies born at St. Boniface Hospital which was reprinted by the Free Press thereby achieving a larger audience.
The family is wonderful, the child simply amazing and much like many of the aforementioned similar stories on Facebook and Twitter inspires people to have hope. We all want in the end to feel good about things rather than dwell in sorrow so when these stories come along we tend to see them in a favourable light rather than critically analyze what they mean in the context of the greater picture. In the article they reference, such children as miracle babies and in many respects this is true. Before I go on I feel the need to point out that I am delighted for Mac’s family and admire their perseverance through many dark days. There is no question that they are a loving family who will love him for the rest of his life and provide a wonderful nurturing environment. The concern I have is that they are in the 5% or less of families that have this experience.
If we look at the article referenced above from the United States which is the largest study to date looking at extremely low birth weight infants the findings were that 95% of those infants who people tried to resuscitate at 22 weeks either died or were left with moderate to severe disabilities. This means 5% survive with only mild or no disability. It is the 5% we tend to hear about in the media and are the ones that create the buzz.
Looking For National Guidance
The fly in the ointment in all of this is that the Canadian Pediatric Society that provides recommendations in such situations is also under fire for its statement on Counselling and Management of Extremely Preterm Birth. In this statement in the recommendations section they state: At 22 weeks’ GA, since survival is uncommon, a non-interventional approach is recommended with focus on comfort care. (Strong Recommendation). In response to this statement a great number of practitioners banded together to write a rebuttal that was published in Pediatrics and Child Health in which they believe that the CPS has created simple rules for complicated decisions as the title of the article suggests. The gist of the article is that gestational age alone is inaccurate and using other prognostic factors in addition to gestational age is a better way of guiding decisions. Factors such as estimated weight and certainty of dates for example should come into the picture. Time will tell how the CPS responds but certainly organizations such as the Canadian Premature Babies Foundation are siding with the authors of the response to the CPS.
Make no mistake, this is a complicated issue and it will not go away anytime soon. While we are not advocating for 22 week infants to be resuscitated routinely, the fact remains if well informed parents decide they want to try it will be difficult to say no. Parents need to understand however that for infants to have the best chance, a coordinated approach with Obstetrics and Neonatology is critical to ensure the best chances. Furthermore seeking the opinion of a Bioethicist would help crystallize some of the issues that I know many are struggling with. Failure to receive antenatal steroids at 22 or 23 weeks for example is clearly shown in this article to reduce the likelihood of a positive outcome. Having a face to face discussion between the Neonatologist and Obstetrician and presenting a unified message to the family will be an imperative first step in any discussion. Furthermore having clear direction in a resuscitation and best practices worked out in the NICU to ensure that skin integrity is maintained is a must. We have a long road ahead of us before we can truly say that we are offering the best chances to these tiny infants but with collaborative efforts between our members in Neonatology and Obstetrics I believe we can get there.
In the meantime we each need to do our part and use our voices (or writing such as this) send a clear message to the public that while we celebrate with the families who have had such great outcomes at these gestational ages we all too often are mourning the loss of the vast majority who were not so fortunate.
Thank you to Dr El-Sayed for providing slides and a great deal of guidance in developing this post!
I am too young a Neonatologist to recall some of the changes in practice that would be considered giant leaps in my field. Provision of antenatal steroids to accelerate lung maturity, development of ventilators and provision of surfactant to premature infants have saved millions of lives the world over and reduced morbidities from the conditions they were designed to treat.
I believe we are embarking on another such tidal wave of change that is beginning to take shape and will come crashing into the shores of our practices globally before long. What makes it all the more exciting is that I have a front row seat to view the birth of this development. The story begins over a decade ago with the understanding that traditional echocardiograms as performed by a Cardiologist in some instances could not provide us as Neonatologists with enough information to guide clinical decision making. Let me state up front that the program I will be discussing would not be possible without the participation of our colleagues in Cardiology and moreover the information that they provide for many infants with congenital heart disease is critical to our practice. What I am referring to though are those instances where we are more interested in the flow of blood or the function of the heart in the presence of a structurally normal heart.
In Canada there is no doubt that Dr. Patrick McNamara has been a pioneer in the field of Targeted Neonatal Echocardiography (TNE) and has published extensively in the field. One such paper from 2009 highlights how TNE can be of use in the treatment of a PDA. TNE though has expanded in use to guide treatment of such conditions as PPHN with or without BPD, heart failure, shock and also point of care functions such as determination of line placements or intravascular clots. Additional work has been done by pioneers in Australia such as Nick Evans. We were very fortunate to have Dr. Yasser El-Sayed train under Dr. McNamara and then return to Winnipeg to develop our own clinical program for TNE in consultation with our colleagues in Pediatric Cardiology.
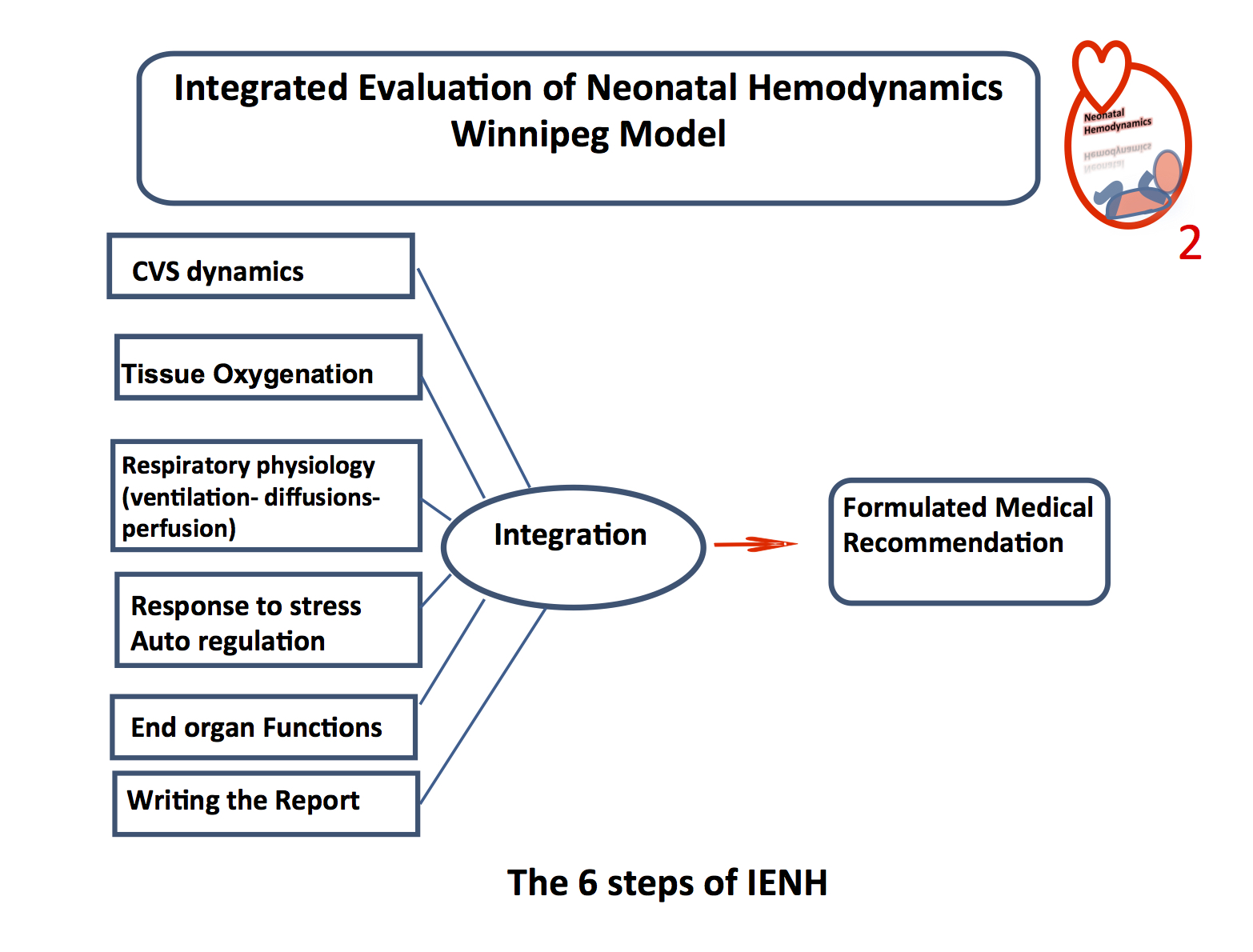
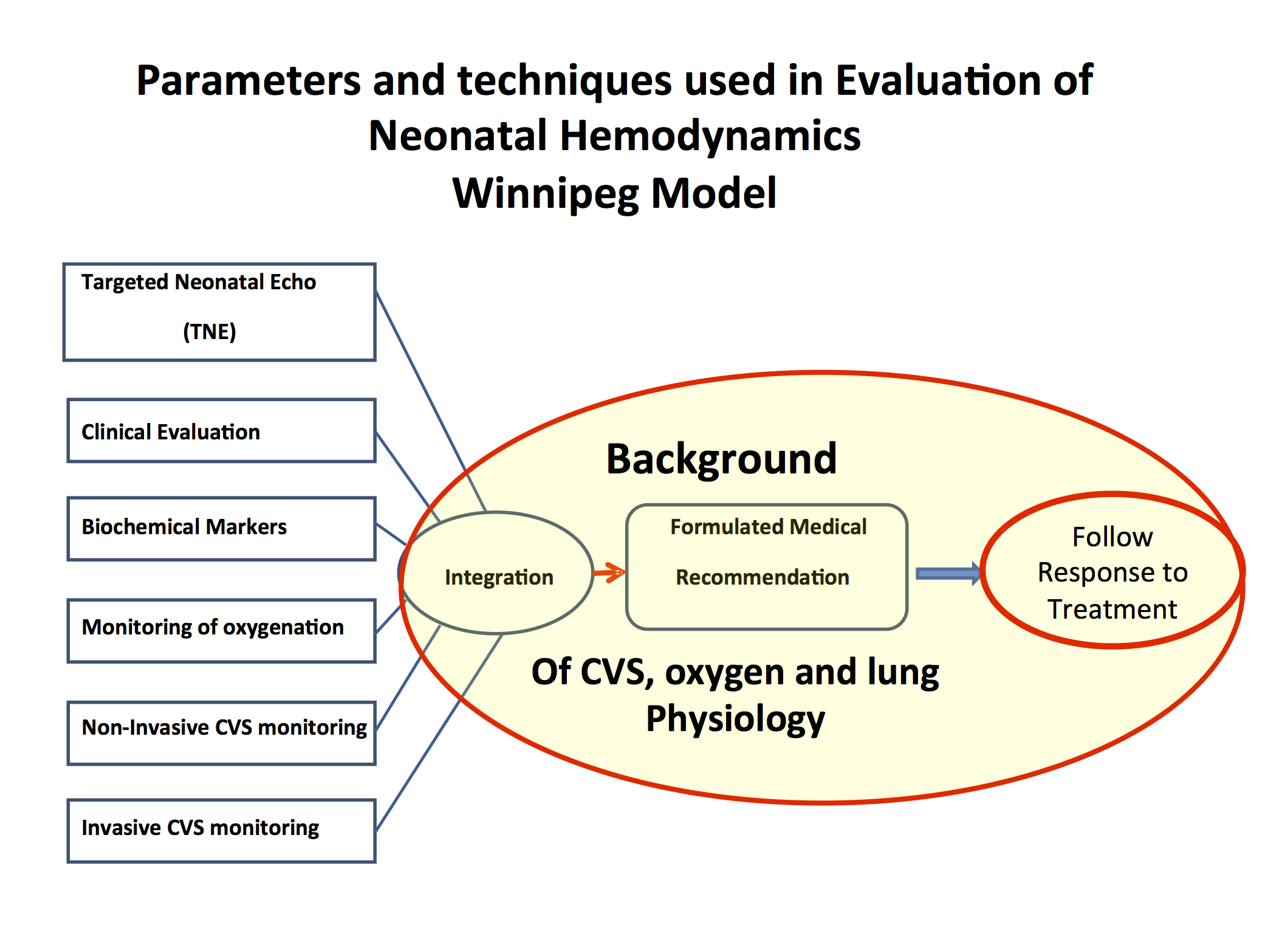
Since it’s inception here the program has been utilized extensively with clinical management in many cases influenced by the findings. We believe though that our program may be unique in the sense that the philosophy of using this technology is only as part of a larger framework as outlined in this figure. The program is known as Integrated Evaluation of Neonatal Hemodynamics (INEH). The concept is that we cannot rely on only one measure of cardiac performance or blood flow patterns. Rather it is through consideration of six separate streams of data that we can come to an accurate conclusion. For example a patient who is hypotensive as defined by a mean blood pressure lower than their gestational age but who has adequate cerebral blood flow as measured by Near Infrared Spectroscopy, normal SVC flow and contractility, as a measure of cardiac performance with a normal lactate and urine output, may need simple observation. Why treat with an inotrope if the end organs are not impaired in the least?
How do we accomplish this is practice? The integration is done by using data as shown in the next figure. Markers such as NIRS, lactate, BNP, indwelling arterial access, urine output all provide useful markers which are integrated to determine the best course of action.
I would like to provide an illustrative case. The patient in this presentation is one who developed hypoxic ischemic encephalopathy. If you read through the slides you will clearly see how the use of INEH brought about a significant change in the approach to the care of the infant. Without this information we would have continued to go down a treatment path which was not addressing the issues at hand appropriately. Please click on the link to view this presentation.
I am proud to say that Dr. El-Sayed is spreading this message and approach globally having recently given workshops in Turkey and Egypt. We are also very excited that in the Fall from October 29th – 31st we will be hosting the 10th Annual Bowman Symposium featuring Neonatal Hemodynamics. For more information please click here.
The importance of this approach to Neonatal Care can not be emphasized enough. With so many needs in our Health Region it is difficult to always obtain enough funds to purchase all the equipment that one needs for a service. As such I was grateful to Dr. El-Sayed for presenting such need at a recent charitable event as shown below!
If you or someone you know is interested in this emerging field we would love to hear from you. If you would like to attend the Bowman Symposium please contact us at:
The picture looks ridiculous. Why does this seem so unnatural yet we feed babies this same product around the world. Granted they don’t drink it from the source as this man is but the liquid is in essence the same. As the saying goes, “Cow’s milk is for baby cows”. When you put it that way it helps put in context the question posed as the title of this post. Should we be surprised that the consumption of a milk meant for another species might have some side effects at a population level if fed to enough infants; especially those with fragile bowel due to prematurity or other high risk condition compromising blood flow to the gut.
The following piece was written by Kari Bonnar with contributions from Sharla Fast both Registered Dieticians in our NICUs. It has been recognized for some time now that the use of donor milk in our highest risk premature infants is associated with less NEC and based on a previous review of the evidence we have been using DBM for the past several years. What this post explores though is the potential for further benefit by taking the next step. That is to ask the question; what additional benefit may be gained by replacing all sources of Cow’s Milk protein in this population. I am delighted to present their review of the literature here as I am sure you will find it as informative and thought provoking as I have.
The health benefits of human milk for all infants, including those born extremely premature, have been increasingly recognized and published.1 The American Academy of Pediatrics policy statement on breastfeeding and the use of human milk recommends that all preterm infants receive human milk including donor human milk if mother’s own milk is unavailable.2 When compared with a diet of preterm formula, premature infants have improved feeding tolerance and a lower incidence of late onset sepsis and necrotizing enterocolitis (NEC) when fed their mothers’ own milk.3 For mothers of extremely premature infants, providing sufficient milk to meet their infant’s needs is a common challenge. Pasteurized donor human milk has been made available to this population in WRHA since 2011 as it has been found to be well tolerated and is also associated with a significantly lower incidence of NEC.4
However, as the sole nutritive substance, human milk does not meet the macronutrient and micronutrient requirements of preterm infants. Multi-nutrient fortifiers are required to provide additional protein, minerals and vitamins to ensure optimal nutrient intake and neurodevelopmental growth.5Prolacta Bioscience has recently launched in Canada with their human milk-based fortifiers, which are gaining popularity due to the ongoing research and success with these products in the United States, Austria, and now Canada.6 It is a new and novel approach that is proving to be most beneficial in reducing neonatal morbidity and mortality rates.7
In infants fed an exclusive human milk diet, Sullivan et al. found a reduction in medical NEC of 50% and surgical NEC of almost 90% compared to a diet containing cow’s milk-based products.7 To date, there is no other intervention that has had such a marked effect on the incidence of NEC.8 Abrams et al. found that for every 10% increase in intake of anything other than an exclusive human milk diet, the risk of NEC increases by 11.8% and the risk of surgical NEC increases by 21%, both with a 95% confidence interval.9
Patel et al. found that for every dose increase of 10ml/kg/day of human milk over the first 28 days post birth, the odds of sepsis decreased by 19%.10 Further to this, they found that overall NICU costs were lowest in very low birth weight (VLBW) infants who received the highest daily dose of human milk. Similarly, Abrams et al. reported that for each 10% increase in the intake of other than exclusive human milk diet, there was an 18% increase in risk for sepsis.9 In addition to predisposing the infant to other morbidities in the preterm population, and subsequent neurodevelopmental disability, sepsis significantly increases NICU costs by 31%. This translates into higher societal and educational costs for VLBW infants who survive sepsis with neurodevelopmental disability.10,11
A reduction in the number of days on total parenteral nutrition (TPN) was found by Cristofalo at al. with the use of an exclusive human milk based diet, in addition to reduction in sepsis and NEC.12 These same findings have been documented by Ghandehari et al. which reflect that an exclusive human milk diet leads to improved feeding tolerance and therefore, a decrease in total TPN days.13 Given that TPN is often the cause of late onset sepsis, the reduction of TPN days is imperative and almost always translates into decreased length of stay.14 Abrams et al. found that duration of TPN was 8 days less in infants receiving a diet containing <10% cow’s milk-based protein versus ≥ 10%, another recognizable dose related finding.9
It is well documented that increased growth leads to a decreased incidence of cerebral palsy and poor neurodevelopmental scores at 18-22 months corrected age, therefore adequate growth (weight, head circumference and length) is crucial in this population.15 The study by Hair et al. followed a standardized feeding protocol with early and rapid advancement of fortification with donor human milk derived fortifier and found that growth standards were being met and resulted in a marked decrease in extrauterine growth restriction.14 Cristofalo et al. study also compared growth rates, which were found to be slightly slower in the human milk fortified versus cow’s milk fortified arm of this study. However, it was mentioned that the small differences could be prevented with further adjustments in fortifier to improve rates of growth, as shown by Hair et al.12, 14 Abrams et al. confirms in their findings that growth rates were similar among human milk-based and cow’s milk-based fortification.9 This is a popular area of ongoing research with many abstracts also showing adequate growth rates with use of human milk-based fortifiers.
In closing, the review of current evidence clearly indicates that a diet of exclusive human milk is associated with lower mortality and morbidity in extremely premature infants without compromising growth and should be considered as an approach to nutritional care for these infants. Further research is needed to fully capture the extent to which using exclusive human milk diets actually reduce overall healthcare costs via improving the short and long term outcomes of extremely premature infants. Research to date only explores the financial impact for the first few years of life; therefore the true costs of these major morbidities are vastly underestimated and underreported. There are many unpublished trials and abstracts that are currently in process that will only strengthen the shift toward exclusive human milk-based diets, ideally making this common practice among Canadian centres in the very near future.
1 American Academy of Pediatrics. Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2005; 115:496-506
2 American Academy of Pediatrics. Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2012; 129:3;e827-41
3 Schanler RJ, Shulman RJ, Lau C. Feeding strategies for premature infants: Beneficial outcomes of feeding fortified human milk vs preterm formula. Pediatrics 1999;103:1150-7
4 Boyd CA, Quigley MA, Brocklehurst P, Donor Breast milk versus infant formula for preterm infants: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed 2007;92:F169-75
5 Agostini C et al. Enteral nutrition supply for preterm infants: commentary from the European society for pediatric gastroenterology, hepatology, and nutrition committee on nutrition. JPGN 2010;50:1:85-91
7 Sillivan S, et al. An Exclusively Human Milk-Based Diet is Associated with a Lower Rate of necrotizing Enterocolitis than a Diet of Human Milk and Bovine Milk-Based Products. J Pediatr 2010:156;562-7
8 Bell EF. Preventing necrotizing enterocolitis: what works and how safe? Pediatrics 2005:115;173-4
9 Abrams SA, Schanler RJ, Lee ML, Rechtman DJ. Greater Mortality and Morbidity in Extremely Preterm Infants fed a diet containing cow milk protein products. Breastfeed Med. 2014:9;1-8
10 Patel AL, Johnson TJ, Engstrom JL, Fogg LF, Jegier BJ et al. Impact of early human milk on sepsis and health-care costs in very low birth weight infants. J Perinatology 2013:33:514-19
11 Ganapathy V, Hay JW, Kim JH. Cost of necrotizing enterocolitis and cost-effectiveness of exclusively human milk-based products in feeding extremely premature infants. Breastfeed Med. 2012:7;29-37
12 Cristofalo EA, Schanler RJ, Blanco CL, Sullivan S, Trawoeger R, et al. Randomized trial of exclusive human milk versus preterm formula diets in extremely premature infants. J Pediatr. 2013;1-4
13 Ghandehari H, Lee ML, Rechtman DJ. An exclusive human milk based diet in extremely premature infants reduces the probability of remaining on total parenteral nutrition: a reanalysis of the data. BMC. 2012:5;188
14 Hair AB, Hawthorne KM, Chetta KE, Abrams, SA. Human milk feeding supports adequate growth in infants ≤1250 grams birth weight. BMC. 2013:6;459
15 Ehrankranz RA, Dusiuk AM, Vohr BR, Wright LL, Wrage LA, et al. Growth in the neonatal intensive care unit influences neurodevelopmental and growth outcomes of extremely low birth weight infants. Pediatrics. 2006.117:4; 1253-61
A judge has granted a man the right to a physician assisted death in Manitoba as reported by the CBC yesterday. Given this landmark ruling based on a change in the Canadian stance allowing such decisions the question turns to children and then neonates. At the present time this stance does not apply to these populations but it is fair to ask the question… what if it did?
The Groningen Experience
As the saying goes “the more things change the more they stay the same”. In 2005 I was but a year into my career as a staff Neonatologist and we were discussing whether we should resuscitate 22 and 23 week infants. Sound familiar? In the back and forth discussion, one of the things that came up from time to time was that the Dutch at least had the option of euthanasia to fall back on if they decided to resuscitate an infant and then the family or care providers changed their minds. It was not necessary to prolong the suffering of the family and patient in the face of futility. I remember being shocked by such a ruling in Holland’s legal system, as euthanizing a newborn in North America was and still is today something that most could not come to grips with. Nonetheless the Groningen protocol as it became known, was introduced in 2004 by Eduard Verhagen the medical director of the department of Pediatrics at the University Medical Center Groningen and became endorsed almost 10 years ago to the day by the Dutch Society of pediatrics.
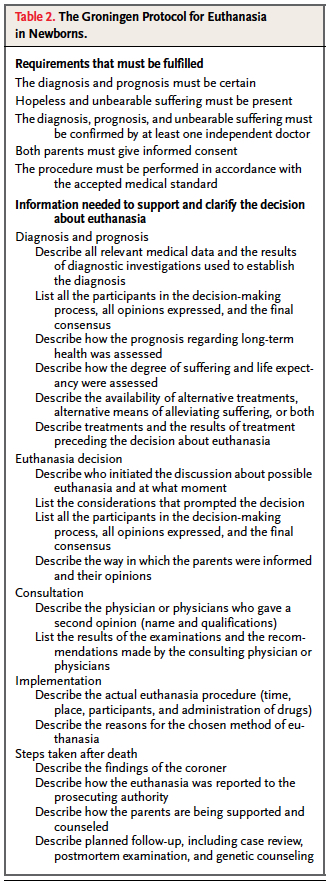
Although many of you may be caught off guard as you read this, it really did generate a fair bit of attention here in North America and has been the subject of many articles and news reports over the years. The Groningen protocol is quite extensive as shown in the table.
The key elements to the protocol are:
(1) diagnosis and prognosis must be certain
(2) hopeless andunbearable suffering must be present
(3) a confirming second opinion by an independent doctor
(4) both parents give informed consent
(5) the procedure must be performed carefully, in accordance with medical standards.
There were some that worried birth at 22 weeks would meet this criteria and lead to ELBW infants being euthanized after a few hours of life rather than using the method of comfort care that we are accustomed to in North America if carrying on seemed futile. Although the outcome is the same, the route to get there is clearly different.
So the question then is what has happened in Holland since this practice was made permissible by the courts? In 2005 shortly after the protocol was introduced, Verhagen published a piece in the NEJM reviewing all the cases of newborn euthanasia from 1997 – 2004. In all there were 22 cases each of which involved a case of spina bifida and in most quite severe. Interestingly there were no cases of premature infants.
What Happened in Holland Over Time
In 2013 he published a a second article in which he acknowledged that worldwide people were concerned that a slippery slope would occur in Holland. As such, he examined all neonatal deaths in NICU from 2005 – 2010. Withholding or withdrawing treatment was the reason for death in 95% of cases. During that period only 1 patient with Osteogenesis Imperfecta type II was classified as euthanasia. This dramatic decline from the pre 2005 state may seem surprising but it is offset by an increase in second trimester terminations after ultrasound at 20 weeks became standard practice in Holland. Previously it was only offered to those over 35 years of age. In fairness, he does acknowledge that there could be underreporting occurring but as he points out, given the lack of consequence in the legal system provided that the protocol is followed there would be little reason to not report as such. There are some cases of paralytic use described in what was classified as withdrawal of support in which the medication was used to treat the gasping efforts of the infant in the last moments of life. While these cases are technically euthanasia, in that the end of life is no doubt hastened, at that point it could be measured in minutes. Is that so wrong if the team views this as distressing to the patient and family. Perhaps yes in some eyes but ask yourself if it is that different from knowingly pushing doses of narcotics higher in the same circumstance which achieves the same end point at times.
So it would seem that the rate did not increase and in fact a marked decrease actually occurred. Curiously a second study has been just released Dutch neonatologists have adopted a more interventionist approach to neonatal care. The study is a joint effort by the Dutch including Verhagen and Dr. Janvier of St. Justine in Montreal who we were fortunate to hear speak recently in Winnipeg. The paper describes a very interesting phenomenon. The authors compared all infants born at > 22 weeks who either died in the delivery room or in the NICU in two epochs; 2001 – 2003 and 2008 – 2010 specifically looking at measures of intervention in the two periods. Would more legal clarity making it permissible to end a life lead to higher mortality in the second period, as a marker of less invasiveness? In both periods there was only one patient that received comfort medication in the delivery room. Furthermore, there were no differences in the number of patients dying in either site. As described in the 2013 paper there were increases in the rate of termination of pregnancy in the second period but there is no support for the argument that the Dutch became less interventionist after the relaxing of laws on euthanasia. Lastly as further evidence that they went the other way, length of stay increased significantly in the NICU from 11.5 to 18.4 days in the second period reflecting less withdrawal in part.
What Conclusions Can We Draw About Our Own Populations?
As the title of this post suggests, it would appear that much of the worry in 2005 has simply not come to pass. Yes there has been a shift to termination for congenital anomalies in the second trimester but that would be no different from our practice in North America. I can’t help but draw parallels between the arguments for the legalization of some drugs such as marijuana and euthanasia. The decriminalization of the former is expected to have the benefit of reducing crime and perhaps even abuse of the drug as it no longer becomes as attractive once it is no longer “sinful”. Has a similar effect happened in Holland perhaps by bringing the discussion to the world stage? It may well be that the change in law in Holland created the opposite effect whereby the Dutch painfully aware that they were being “watched” became even more reluctant to hasten the time of death in these situations. There is no doubt that something changed after 2005 as they became more interventionist and not less.
A final thought has to do with a thought that Dr. Verhagen raises in the 2013 piece. Has the transition to a model of terminating pregnancies in the second trimester been a good or bad thing. He argues that ultrasound is not as predictive in terms of diagnosis as examining a patient after birth. When an infant is in front of your eyes, facial features combined with enhanced imaging may reveal a change in diagnosis compared to what is determined antenatally. Similarly, a patient with a seemingly inoperable heart defect may have a slightly different scan after delivery which provides some options for the family. If examination after birth is superior to antenatal diagnosis in terms of accuracy, are we doing the right thing by forcing families to decide on termination prior to delivery? In Holland the option exists although clearly not being taken to assess a patient after birth and then if the diagnosis meets the Groningen protocol a life can be ended early. It can be argued of course that euthanasia is not the only option and that one can choose not to feed and withdraw life-sustaining treatment.
The question that I will leave you with though is as a parent would you want to watch your infant die after 5-7 days dehydration or end their life given the outcome is the same on the same day you choose “compassionate care”? Which is the more humane decision when the outcome is the same?



 The integration is done by using data as shown in the next figure. Markers such as NIRS, lactate, BNP, indwelling arterial access, urine output all provide useful markers which are integrated to determine the best course of action.
The integration is done by using data as shown in the next figure. Markers such as NIRS, lactate, BNP, indwelling arterial access, urine output all provide useful markers which are integrated to determine the best course of action.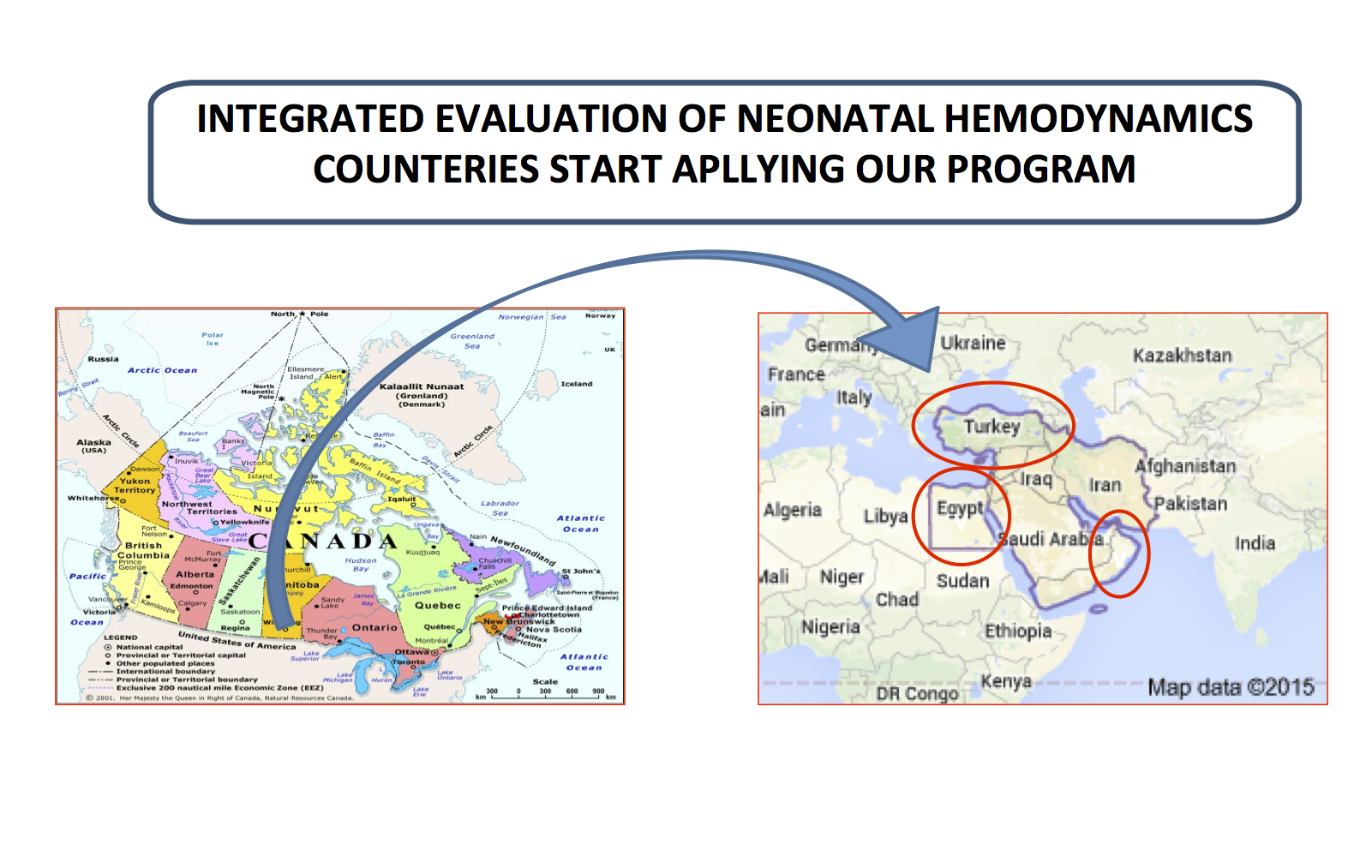
 We are also very excited that in the Fall from October 29th – 31st we will be hosting t
We are also very excited that in the Fall from October 29th – 31st we will be hosting t